


Abstract
Background Sacroiliac joint fusion (SIJF) has been established as an effective treatment for sacroiliac joint dysfunction. However, failure necessitating revision has been reported in up to 30% of cases. Little is known regarding outcomes of revision SIJF.
Methods We retrospectively reviewed all revision SIJF at a single academic center between 2017 and 2020. Revision surgery was performed using the principles of joint decortication, bone grafting, compression, and rigid internal fixation. Outcomes were assessed at 6 months and 1 year after surgery using the Oswestry Disability Index (ODI), Numeric Pain Rating Scale (NPRS), and Single Assessment Numeric Evaluation (SANE) scale. Fusion was assessed using computed tomography at 12 months postoperatively.
Results Eighteen revision SIJFs in 13 patients were included. The mean age was 55.8 years (range 35–75). Mean body mass index was 27.9 (range 21.7–36.7). Sixty-two percent of the patients were women. The indications for revision were pseudarthrosis without fixation failure in 14 cases (77.8%), hardware failure (loosening) in 3 cases (16.7%), and continued pain after partial fusion in 1 case (5.6%). ODI and NPRS scores demonstrated significant statistical and clinical improvements at all timepoints. Mean (SD) ODI scores improved from 53.8 (19.9) preoperative to 37.5 (19.8) at 6 months and 32.9 (21.7) at 12 months. Improvement in ODI was found in 15 joints (83.3%), and the minimal clinically important difference (MCID) was achieved in 12 joints (66.7%). Mean (SD) NPRS scores improved from 6.5 (1.4) preoperative to 3.2 (2.8) at 6 months and 3.4 (2.6) at 12 months. Improvement in NPRS was also identified in 17 joints (94.4%), and 10 joints (55.6%) achieved MCID for NPRS. Mean (SD) SANE score was 72.0% (30.8) at 6 months and 70.0% (33.8) at 12 months. There were no radiographic lucencies, implant subsidence, or implant fractures at final follow-up. We identified an 88.9% fusion rate with definitive bridging bone across the sacroiliac joint.
Conclusion Utilizing a principles-based technique of joint decortication, compression, and rigid internal fixation, revision SIJF showed an improvement in patient-reported outcomes as well as high rate of fusion at 12 months. The most common indications for revision SIJF are symptomatic pseudarthrosis and implant loosening. This is the largest series of revision SIJF to date.
Level of Evidence 4.
- sacroiliac joint
- SI joint
- SIJF
- sacroiliac joint dysfunction
- sacroiliac joint fusion
- back pain
- decortication
- compression
- internal fixation
- revision
Introduction
Sacroiliac joint dysfunction (SIJD) is an increasingly recognized source of low back pain. Within patients presenting to a physician for back pain, the sacroiliac joint (SIJ) has been identified as a contributing or predominant factor in many patients.1–6 Nonoperative management remains first line; however, SIJ fusion (SIJF) is often pursued for recalcitrant symptoms.2,7–12
SIJF, particularly minimally invasive SIJF, has been demonstrated as a viable treatment option for activity-limiting SIJD. Previous investigations have shown improved patient-reported outcomes, functional improvements, quality of life, and radiographic outcomes after SIJF when compared with nonoperative management.11,13–21 Published reports state revision rates between 0% and 30% depending on the method of fixation and patient-related factors.14,19,22–24 However, modern SIJ-specific implant systems have demonstrated low revision rates between 2.1% and 6.7%.14,19,25–27 Common mechanisms of failure include implant malposition and symptom recurrence secondary to pseudarthrosis and/or implant failure.
While there have been numerous investigations demonstrating excellent clinical outcomes after primary SIJF, there remains a paucity of data on the outcomes after revision SIJF. Therefore, the purpose of this study is to (1) describe the authors’ technique for minimally invasive revision SIJF, (2) determine the patient-reported outcomes after minimally invasive SIJF, and (3) determine the radiographic outcomes after revision SIJF.
Methods
Between January 2017 and May 2020, all cases of revision SIJF performed by a single surgeon at a single institution were identified. Patients aged <18 years and those with <12 months of clinical follow-up, revisions for malpositioned instrumentation, or concomitant lumbar procedures at the time of SIJF (including instrumentation removal) were excluded. All patients were implanted with an SIJF system (Integrity SIJ Fusion system with Blade-X Technology, OsteoCentric Technologies, Logan, UT) that utilizes the surgical principles of aggressive joint decortication, percutaneous autografting, compression across the SIJ with rigid internal fixation, and a fenestrated design allowing ingrowth across the SIJ and through the implant. All patients were followed clinically for at least 12 months postoperatively with clinical and radiographic evaluation at 6 and 12 months. Pelvis computed tomography (CT) images were routinely obtained at 12 months postoperatively to assess fusion. Patients filled validated patient-reported outcome measurements: the Oswestry Disability Index (ODI), Numeric Pain Rating Scale (NPRS), and Single Assessment Numeric Evaluation (SANE) Scale. The minimal clinically important differences (MCIDs) used for the ODI and NPRS were 10 and 2, respectively.28
Arthrodesis was assessed via CT image and confirmed under the following criteria: (1) bridging fusion mass across the SIJ in >2 consecutive 2-mm cuts, (2) lack of peri-implant halo, and (3) lack of hardware breakage. Fusion assessment was classified using a previously described graded scale: Grade 1, no evidence of bone growth across the SIJ; Grade 2, bone growth evident but no definitive bridging bone identified; and Grade 3, bone growth clearly demonstrated bridging the SIJ.29 Last, all CT images were critically reviewed by the authors and a musculoskeletal radiologist for implant loosening, subsidence on the iliac or sacral sides of the SIJ, or neural foramen penetration.
Patient Evaluation
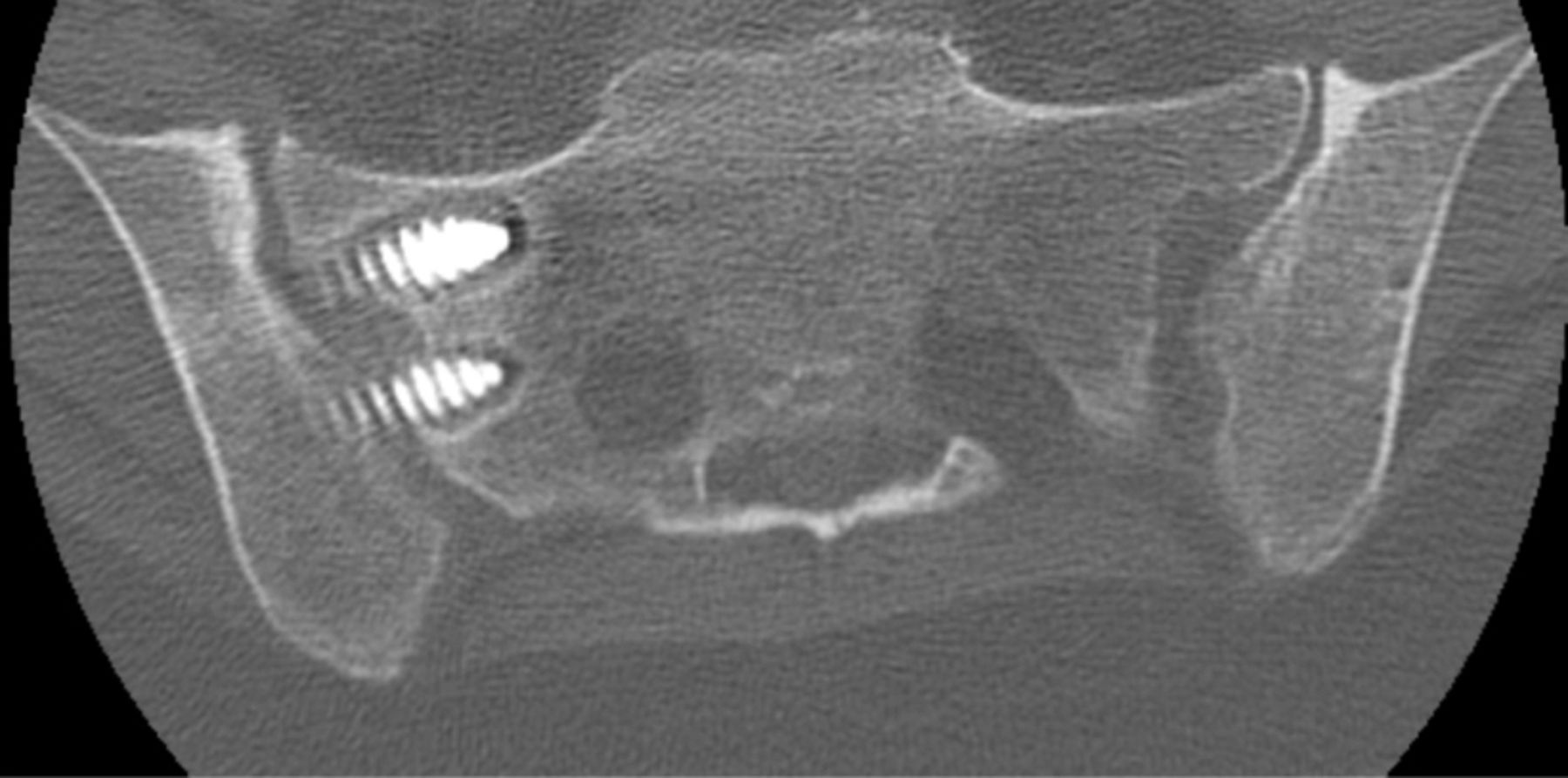
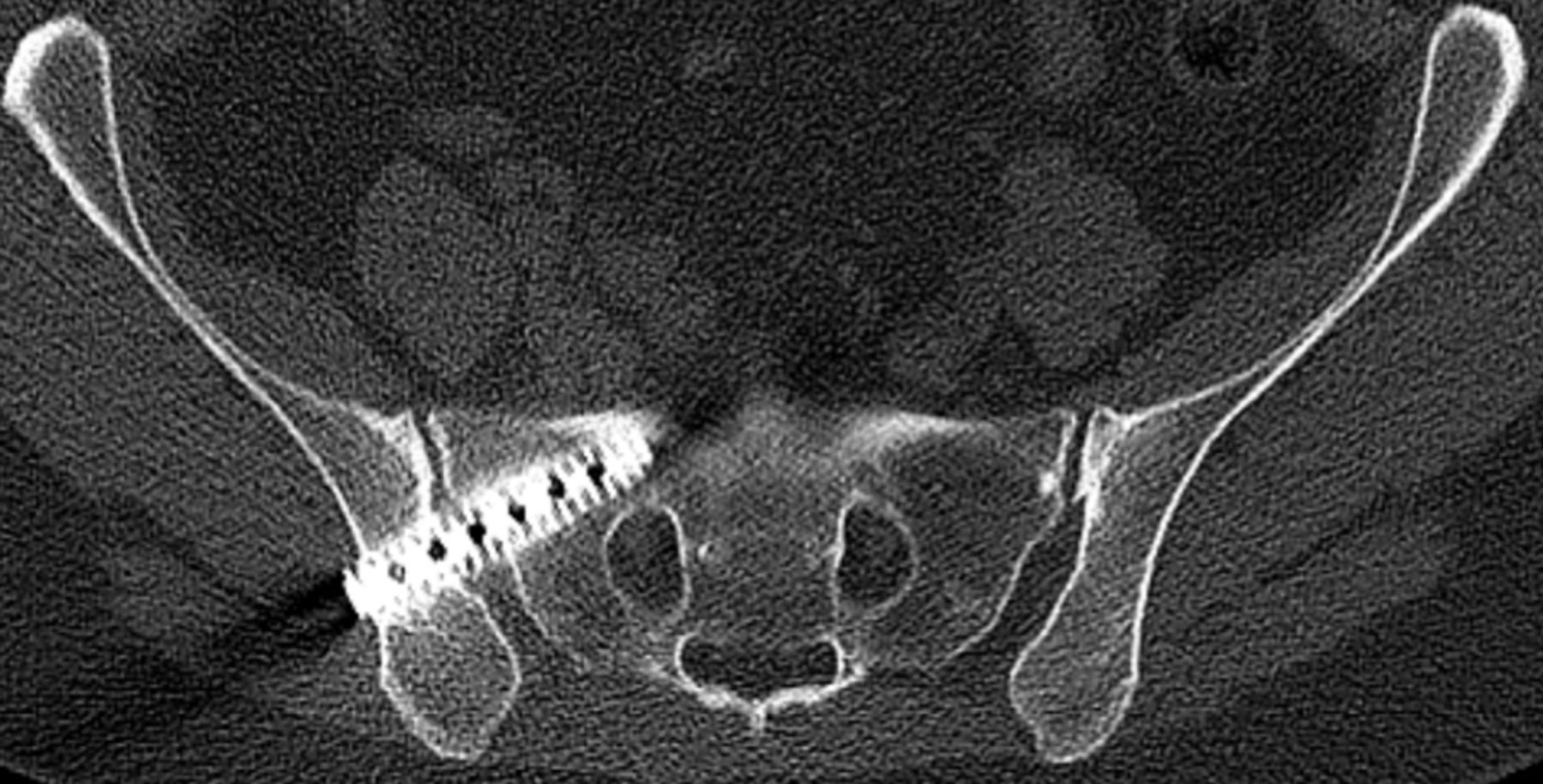
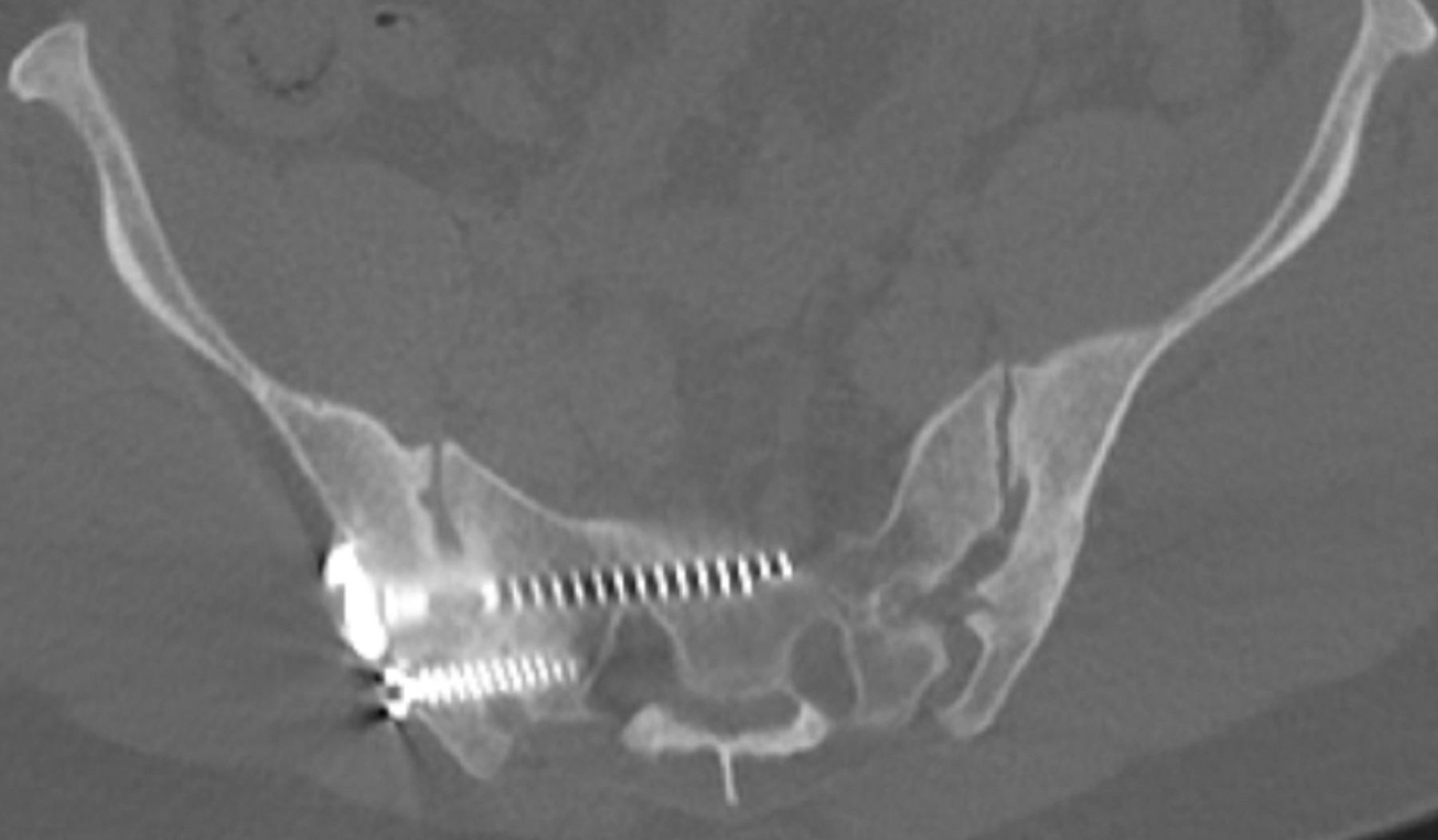
Our evaluation for pain after SIJF includes a patient history, physical examination, radiographic evaluation including pelvis CT without contrast, and, in most cases, diagnostic injection. The details regarding preoperative symptoms, date of primary SIJF, postoperative symptoms, and current presenting symptoms were obtained. Patients were candidates for revision SIJF if specific criteria were met. First, the patient must have signs and symptoms consistent with SIJ-mediated pain. Common historical signs and symptoms include pain located over the buttocks with radiation to the posterior thigh as well as recurrence of symptoms after initial postoperative resolution. Patients must also have ≥3 physical examination maneuvers consistent with SIJ-mediated pain. Physical examination maneuvers include pain with direct posterior superior iliac spine (PSIS) palpation, PSIS distraction, flexion abduction external rotation (FABER) test, Mayo SIJ test (FABER/PSIS distraction combined test), and Gaenslen test.2,3,30 Second, patients must have radiographic evidence of failure of previous SIJF instrumentation or pseudarthrosis. Hardware failure included broken instrumentation and/or hardware loosening (Figure 1). The criteria as suggested by Fogel et al to define pseudarthrosis were used. This is described as (1) absence of bridging bone across the joint surface in 2 consecutive slices on thin-cut CT, and/or (2) evidence of instrumentation breakage or migration31 (Figures 2–3). Third, if pain was not deemed to be from implant malposition, patients underwent diagnostic, local anesthetic-only image-guided (CT or fluoroscopy) injection of the SIJ. Overall, patients must have radiographic and physical examination findings that correlate with the patient’s presenting pain syndrome.

Loosening of sacroiliac joint instrumentation with gross halo and no evidence of bridging bone through the sacroiliac joint.

Sacroiliac joint (SIJ) fusion with author’s described technique (left SIJ). Right SIJ shows pseudarthrosis without instrumentation failure.

Pseudarthrosis without bridging bone through the sacroiliac joint without instrumentation loosening.
Surgical Technique
Minimally invasive revision SIJF was performed in the prone position under general anesthesia. The patient’s previous incision was reopened if amenable to the revision approach, and intraoperative fluoroscopy was used to identify the previous instrumentation. We typically used a 0.062-inch Kirschner wire (K-wire) to cannulate the previous instrumentation. If the implant company and model were known preoperatively, an instrumentation removal set from the company was used to assist with removal. Otherwise, a standard hardware removal set with cannulated screwdrivers and/or trephines was used for implant removal. If the implant was unable to be easily cannulated, a tubular retractor system (MAST Quadrant System, Medtronic, Minneapolis, MN) was used to expose the previous instrumentation for direct visualization and implant removal. It was not uncommon that the previous instrumentation was grossly loose in the setting of pseudarthroses or instrumentation failure. Common findings were ilium ingrowth and a loose sacral implant.
Once the previous instrumentation was removed, the minimally invasive SIJ fusion was used. Utilizing inlet, outlet, and lateral fluoroscopy, a 3.2-mm K-wire was placed across the SIJ in the intended trajectory and position of the implant. The inner and outer tables of the ilium as well as the sacral aspect of the SIJ were drilled with a 12-mm-deep fluted drill. A deployable, rigid blade was then used to aggressively decorticate the SIJ. The fusion zone was then irrigated, and joint debris suctioned out, and a combination of autograft and bone graft extender was placed percutaneously into the void. The autograft was obtained from the 12-mm-deep fluted drill with an average yield of 1 to 4 cc. Bone graft extenders typically included 5 cc of demineralized bone matrix (AlloSync, Arthrex Inc, Naples, FL, USA) and 1.05-mg recombinant bone morphogenetic protein-2 (Infuse, Medtronic, Minneapolis, MN, USA). The bone morphogenetic protein-2 was used off-label and only after patient consent. The 3.2-mm K-wire was then replaced in the intended screw trajectory and the fusion implant placed over this wire. Every effort was utilized to have the implant engage the dense bone in the vertebral body of the S1 or S2 sacral segment (most typically S1), depending on any elements of sacral dysmorphism.32–34 The implant utilized a 10-mm or 12-mm lag screw design, and compression across the SIJ was confirmed with fluoroscopic imaging. The antirotation screw was then placed distal to the implant in a trajectory parallel to the implant, stopping just short of the S1 foramen. Final implant seating and adequate compression across the SIJ were verified by using an anterior-posterior view with a 20° to 40° tilt to match the slant of the pelvic outer table.
Statistical Measures
The statistical analysis was performed utilizing BlueSky 7.4.0 software (BlueSky Statistics Inc., Chicago, IL, USA). Continuous variables were reported as means with ranges or SDs. Group numeric values were compared utilizing the Student t test for parametric values and the Kruskal-Wallis for nonparametric distributions. Categorical variables were assessed with the χ 2 test, or the Fisher’s exact test, given low counts of certain comparisons. For all data points, statistical significance was achieved when the P value was less than 0.05.
Results
Demographics
A total of 21 revision SIJFs performed in 15 patients were included in the study period. Three joints in 2 patients were excluded from the sample. One patient underwent concomitant lumbar instrumentation removal at the time of revision bilateral SIJF, and 1 patient underwent revision for instrumentation malposition, causing neurologic compression. There was an additional patient who developed a pseduarthrosis whose SIJF implant did not cross the SIJ. This failure was classified as a pseduarthrosis and not an implant malposition, since the primary reason for revision was his painful pseduarthosis, not neurologic compression from the malpositioned implant. Thus, our analysis included 18 revision SIJFs. There were 5 bilateral revision SIJFs, 3 of whom underwent simultaneous, single-anesthetic bilateral revision SIJF. The mean age was 55.8 years (range 35–78) (Table 1). Mean body mass index was 27.9 (range 21.7–36.7). Sixty-two percent of the patients were women. Seven patients had previous spine surgery, 6 of whom had previous lumbar fusion. All patients were nonsmokers for at least 6 weeks prior to surgery. Two patients had previously undergone a revision SIJF prior to this reported revision.
Patient demographics.
Indications for Revision
The indications for revision surgery were pseudarthrosis without fixation failure in 14 joints (77.8%), hardware failure (loosening) in 3 joints (16.7%), and continued pain after partial fusion in 1 joint (5.6%) (Table 2). The interval between primary and revision surgery was 27.6 months (range 5–106 months). Of those who underwent revision for pseudarthrosis without fixation failure, with fixation failure, and partial fusion, the interval was 24.5 months (range 5–85 months), 15.7 months (range 5–29 months), and 106 months, respectively.
Indications for revision surgery.
Patient-Reported Outcomes
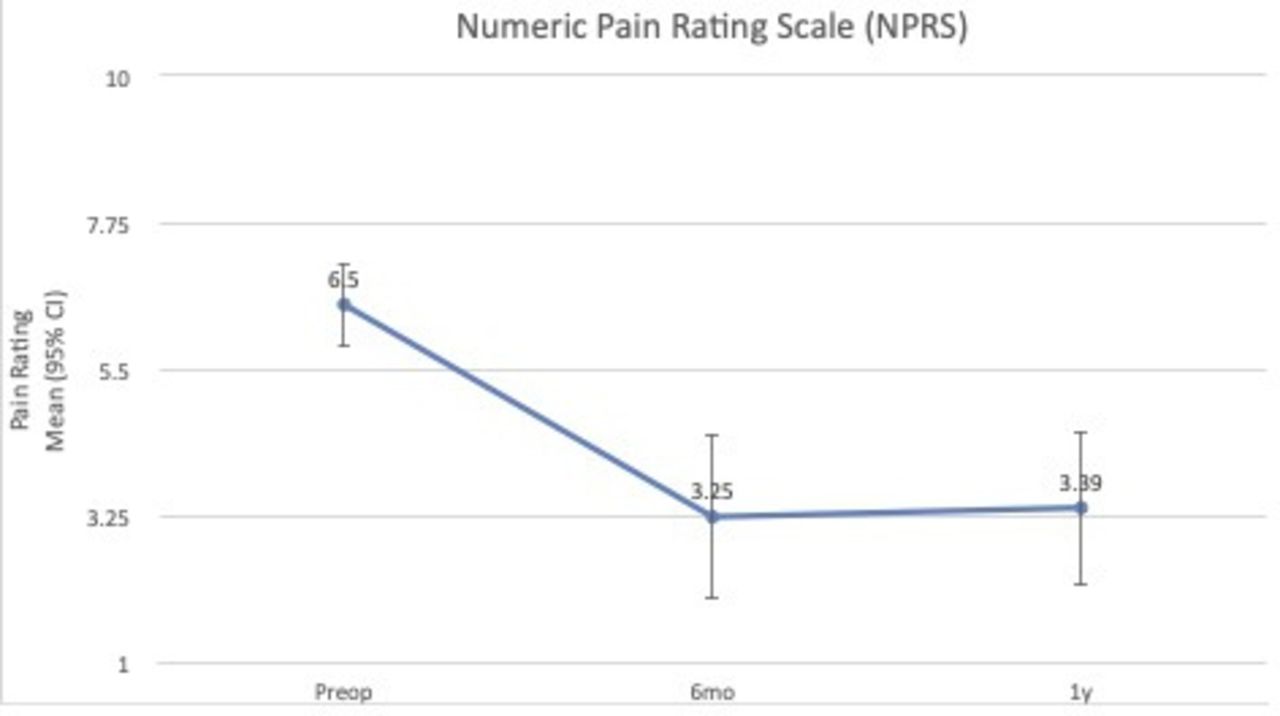
ODI and NPRS scores demonstrated significant statistical and clinical improvements at all postoperative timepoints (Figures 4 and 5). Mean (SD, 95% CI) ODI scores improved from 53.8 (19.9, 95% CI 44.6–63.0) preoperatively to 37.5 (19.8, 95% CI 28.1–47.0) at 6 months and 32.9 (22.7, 95% CI 22.2–43.7) at 12 months (P < 0.001). Improvement in ODI was found in 15 cases (83.3%), and the MCID was achieved in 12 cases (66.7%). Mean (SD, 95% CI) NPRS scores improved from 6.5 (1.38, 95% CI 0.6–7.1) preoperatively to 3.2 (2.8, 95% CI 1.28–4.45) at 6 months and 3.4 (2.6, 95% CI 1.2–4.6) at 12 months (P < 0.001). Improvement in NPRS was also identified in 17 cases (94.4%), and 10 cases (55.6%) achieved MCID for NPRS. Mean SANE (SD) was 72.0% (30.82) at 6 months and 70.0% (33.83) at 12 months. There was no association between patients with previous spine surgery or indication for revision and achieving MCID in ODI and NPRS.
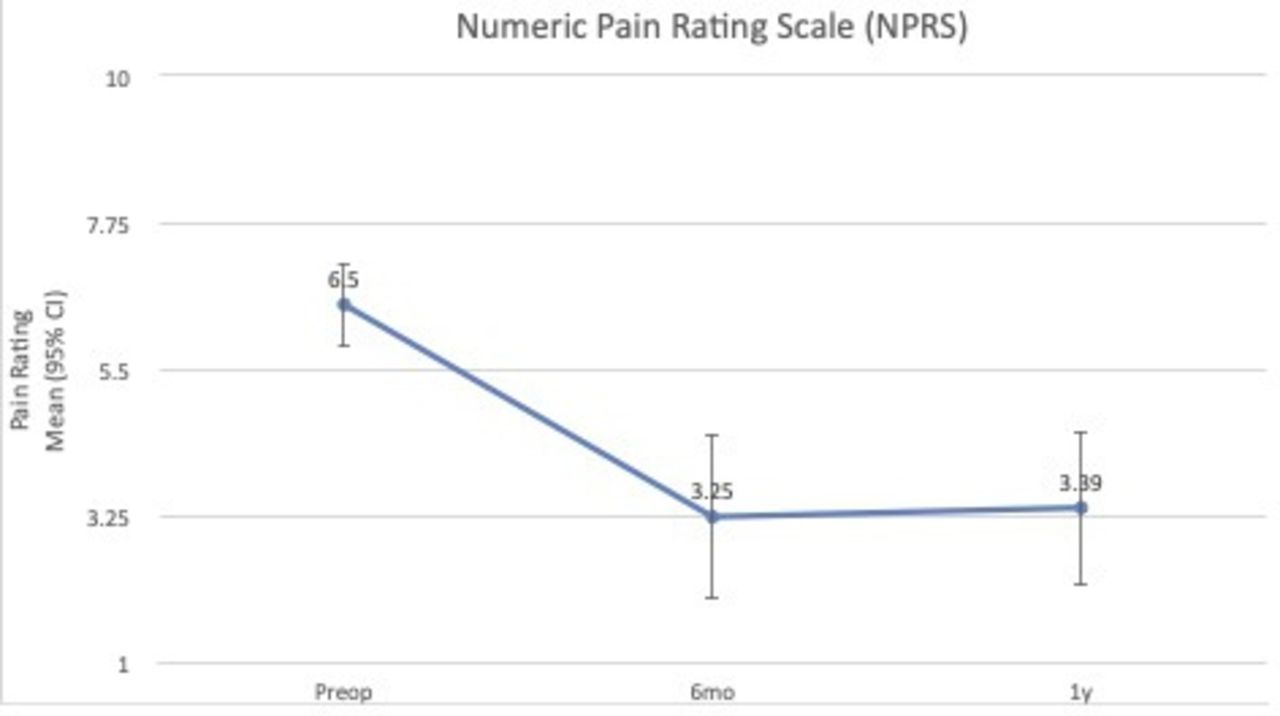
Numeric Pain Rating Scale scores; P < 0.001. Abbreviation: Preop, preoperative.

Oswestry Disability Index scores; P < 0.001. Abbreviation: Preop, preoperative.
Radiographic Outcomes
Postoperative CT image at 12 months was available for 17/18 (94%) of cases. There were no radiographic lucencies, implant subsidences, or implant fractures that occurred at 12 months postoperative (Table 3). We identified an 88.9% fusion rate with definitive bridging bone across the SIJ (Figures 3 and 6). A single case (5.6%) demonstrated bone growth without definitive bridging fusion mass. There were no cases of absent bone growth. The authors and attending radiologist demonstrated agreement on evaluation of fusion status on all cases.
CT fusion grade.

Sacroiliac joint fusion with definitive bridging bone through the sacroiliac joint.
Complications
There were no serious procedure-related adverse events. There were no revision surgeries in the cohort.
Discussion
This review represents the largest clinical series of revision SIJF to date and demonstrated clinically and statistically significant improvement in patient-reported outcomes and an 88.9% rate of fusion in 18 SIJs 1 year after revision SIJF. Our surgical principles emphasize joint decortication, compressions, and rigid internal fixation. Patients experienced a 42.2% improvement in mean ODI and a 47.8% improvement in mean NPRS. Patients reported a mean SANE score of about 70%. In other words, patients reported 70% improvement of their SIJ-related pain at 1 year after surgery. Eighty-three percent of patients reported improvement in ODI, and 66.7% met the MCID for ODI.28 Likewise, 94.4% of patients reported improvement in NPRS, with 55.6% meeting MCID for NPRS. The most common indication for revision was pseudarthrosis without fixation failure (77.8%) followed by fixation failure (16.7%) and partial fusion with recurrent pain (5.6%). There were no surgical complications of infection, hematoma, thrombosis, implant malposition, implant failure, or revision surgery within the study period.
Although there are randomized controlled trials and retrospective studies observing outcomes after primary SIJF, there are few previous studies reporting the outcomes of revision SIJF. At the time of this study, data regarding revision SIJF were limited to case reports, technique guides, and cadaver biomechanical reports, with the current largest published series regarding outcomes of revision SIJF is 7 cases. Cognetti et al reported on their series of 5 patients who underwent revision SIJF utilizing a minimally invasive approach.27 The indications for revision were implant malposition with lumbar radiculopathy in 1 patient and pseudarthroses with recurrence of pain in the remaining 4 patients. All patients reported satisfaction and pain improvement after the revision procedure. However, 2 patients reported low back pain that was dissimilar from their presenting SIJ-mediated pain. The authors did not obtain patient-reported outcomes but did note “interosseus bridging” on follow-up CT 2 years after surgery in all patients. MenMuir et al published a series of 4 patients who underwent minimally invasive revision SIJF with a technique that utilized decortication and a threaded implant.26 All patients were revised for loss of fixation and continued pain. The authors reported that all patients had resolution of prerevision symptoms. However, patient-reported and functional outcomes were not measured, and only 1 patient obtained a postoperative CT image, confirming fusion. Sayed et al reported on the use of a minimally invasive posterior approach SIJF device (Linq [PainTeq, Tampa, FL, USA]) as a salvage of failed lateral SIJF in 7 patients.35 The authors reported a mean NPRS improvement from 8 to 2 at final follow-up. Details regarding the indication for surgery were not included, and there was no formal evaluation of radiographic fusion prior to or after the revision procedure. Additionally, the follow-up was limited to 10 months. However, the authors did report on a single patient who showed postoperative bridging fusion mass after revision procedure. A potential confounder in this study is that 5 of the 8 authors are paid consultants for the device discussed.
There is a growing body of literature describing the outcomes after primary SIJF. While studies generally report good outcomes, there is a subset of patients who experience continued, recurrent, or new pain after SIJF. This postoperative pain may be related to an incomplete diagnosis, implant malposition, surgical technique, and/or lack of fusion. Revision surgery has been reported to be relatively rare but dependent on surgical technique. In a retrospective review of 312 patients treated with multiple 7.2-mm screw fixation vs triangular titanium implants, Spain et al found a 4-year cumulative revision rate of 30.8% after fixation with screws alone and 5.7% after fusion with triangular titanium implants. It should be noted that screw group had no joint preparation prior to screw placement.24 The indication for revision was implant loosening in the screw fixation group and implant malposition in the triangular implant group. Mitchell et al described an increased rate of implant loosening when implants only have purchase in the sacral alar bone compared with implants with purchase in the more dense sacral body.36 Claus et al reported a 6.1% revision rate after SIJF using threaded implants secondary to implant loosening, pseudarthrosis, and persistent pain. Once again, there was no joint preparation in the screw group.37 Review studies have reported overall revision rates at approximately 3.8% at 2 years.38 The most common indication for revision was pseudarthrosis without fixation failure (71.4%) followed by fixation failure (14%), implant malposition (9.5%), and partial fusion with recurrent pain (4.7%). Patients under each indication for revision experienced continued, recurrent, or new pain after primary SIJF, positive SIJ physical examination maneuvers, and positive response to diagnostic SIJ injection. Thus, we identified that the patients’ pain continued to originate from the SIJ, particularly in the group with lack of bridging bone but no evidence of implant loosening.
Controversy and tremendous variability exist regarding the technique and method of fixation for SIJF. Growing acceptance and advances in the treatment of SIJD has led to the development of a wide variety of SIJF devices with various techniques.39 Specific controversies include lateral vs posterior approach, transfixion vs arthrodesis, fixation into the sacral alar vs sacral body, and the use of decortication. The author’s preference is for a technique that emphasizes the arbeitsgemeinschaft für osteosynthesefragen bone healing and fusion principles of (1) bone surface preparation, (2) bone grafting, (3) compression through the fusion surfaces, and (4) rigid internal fixation.40–44 It is also the author’s preference to perform SIJF through a soft-tissue-friendly minimally invasive lateral approach and with implants that engage the denser midline sacral body opposed to the less dense sacral alar bone.
Fusion was identified in 88.9% of joints using the aforementioned principles. These fusion results compare positively to what is published in the primary SIJF literature, even with a technique that incorporates joint decortication. Duhon et al and Dengler et al reported bridging bone across the SIJ in 25% and 35% of patients at 12 months after primary SIJF using triangular titanium implants.45,46 Conversely, Kucharzyk et al, Cross et al, Kube et al, and Abassi et al reported 68.7%, 78.9%, 88.2%, and 73.7% fusion rates at 12 months, respectively, utilizing a technique that included SIJ decortication and a threaded implant.29,47–49 Thus, it is the author’s preference to approach the SIJF procedure utilizing joint decortication, compression, and rigid internal fixation through a soft-tissue-friendly minimally invasive lateral approach.
There are several limitations of this study. First, this is a retrospective, single-institution and single-surgeon case series. As such, there are some nuances to patient selection, and bias may have influenced our outcomes. Second, there is a lack of a control group to other SIJF techniques/implants and conservative management. Third, there is a relatively small sample size, which may lead to underpowered results. However, this is the largest series on revision SIJF yet reported. We attempted to minimize patient selection variability by excluding patients with concomitant spinal procedures and those revised for implant malposition, causing neurologic compression. It is important to note that our study still demonstrated statistical improvement of all reported patient-reported outcome measurements; however, there could be additional findings that remain undetected. Fourth, given the single surgeon and tertiary referral nature of the practice, the results are likely influenced by our singular study protocols, evaluation, and management, which may not be as generalizable to other practice types.
Conclusion
Revision SIJF, utilizing a principles-based technique of (1) joint decortication, (2) bone grafting, (3) compression, and (4) rigid internal fixation, shows improvement in patient-reported outcomes as well as high rate of fusion at 12 months. The most common indications for revision SIJF are symptomatic pseudarthrosis and implant loosening.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosures William W. Cross III is a paid consultant and receives royalties from Osteocentric outside the submitted work. The remaining authors have no disclosures.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.