


Article Figures & Data
Figures
- Figure
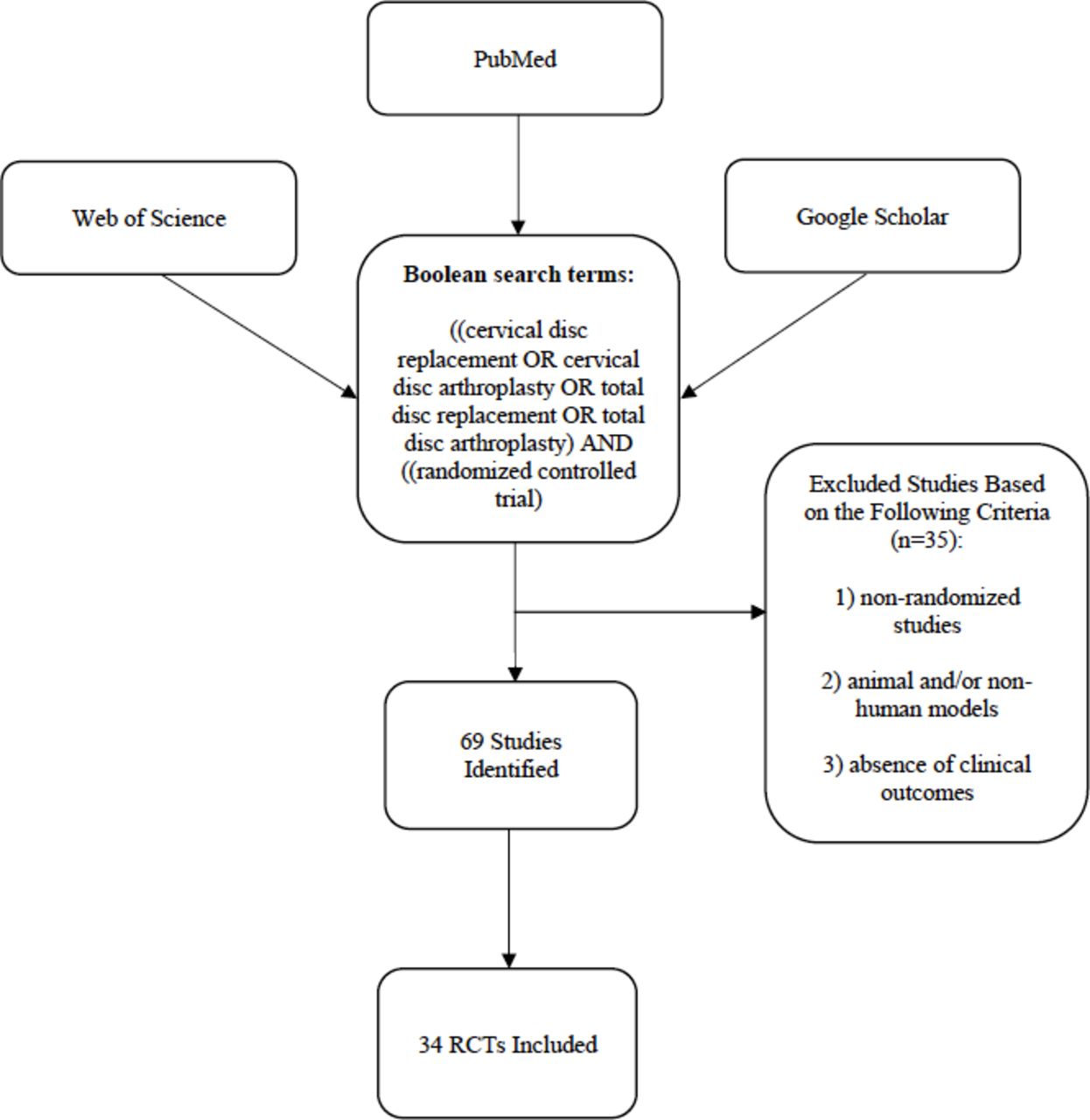
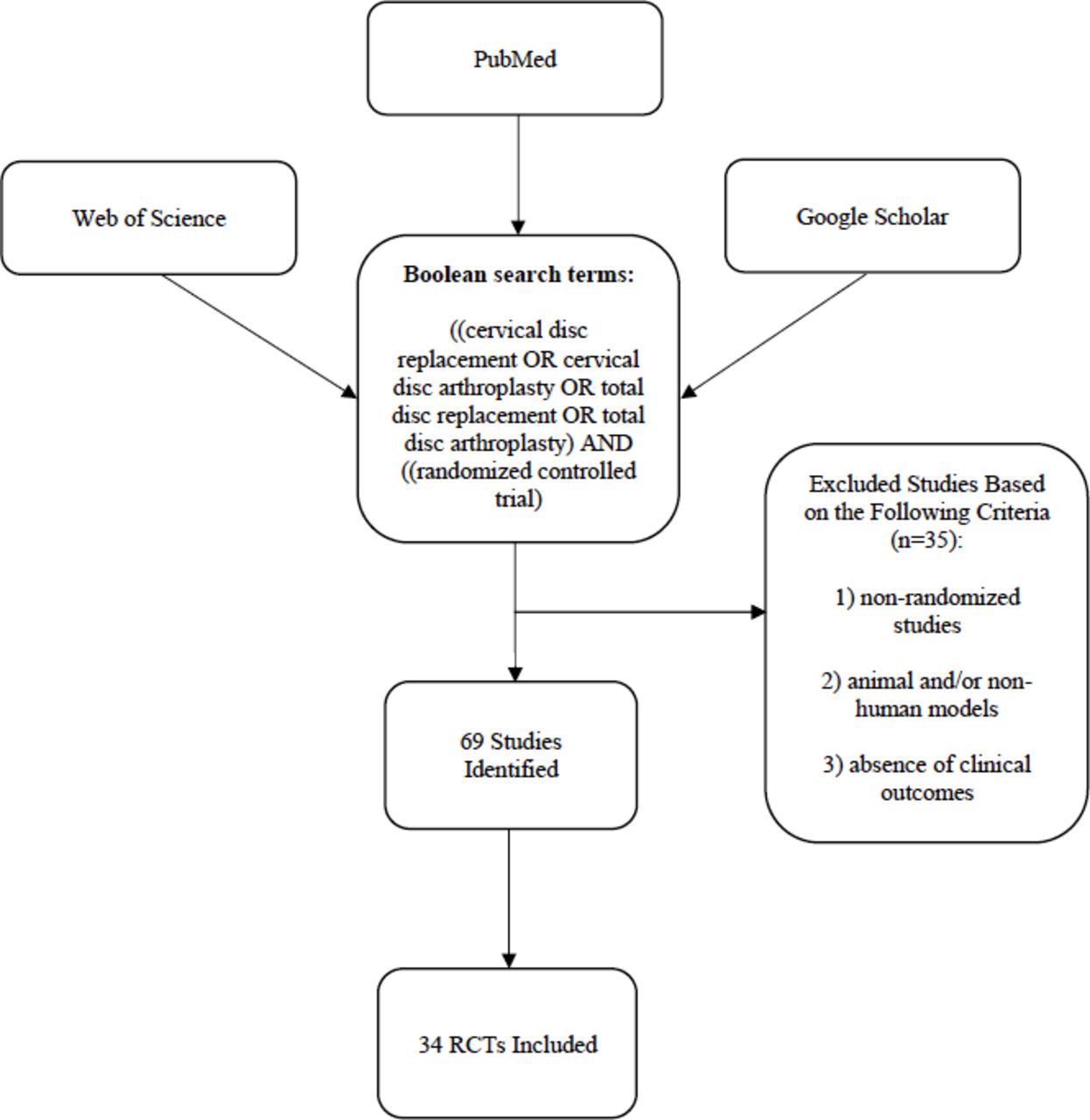
Flowchart of recorded articles related to randomized controlled trials comparing cervical disc arthroplasty to anterior discectomy and fusion.
Tables
- Table 1
Summary of current FDA-approved cervical disc arthroplasty devices with clinical and radiographic image examples.
Implant Name and Manufacturer Picture and X-ray of Implant Articulating Materials Theoretical Center of
RotationInternal Fixation Year Approved by FDA FDA Approved for:
Single/2 LevelMRI Compatiblea: Available Disc Heights (mm) Commercially Available Prestige LP—Medtronic 

Titanium ceramic Superior vertebra Screws 2014 Yes Yes Yes 5, 6, 7, and 8 Yes Bryan—Medtronic 

Titanium-aluminum-vanadium alloy Within implant Milled bone 2009 Yes No Yes 8.5 Yes Prodisc-C—Centinel Spine 

Cobalt-chrome-molybdenum Inferior vertebra Keels 2007 Yes No Yes 5, 6, and 7 Yes M6—Spinal Kinetics 

Titanium-aluminum-vanadium alloy Inferior vertebra Serrated fins 2019 Yes No Conditional Maximum spatial gradient magnetic field of <4000 Gauss/cm (40 T/m)b
6 and 7 Yes Simplify—Simplify Medical 

Polyetheretherketone and porous titanium plasma coating Variable Serrated fins and teeth 2020 Yes Yes Yes 4, 5, and 6 Yes Secure-C—Globus Medical 

Cobalt-chrome-molybdenum “Natural” Serrated keels 2012 Yes No Conditionalb Maximum spatial gradient magnetic field of <4000 Gauss/cm (40 T/m)
7, 8, 9, 10, 11, and 12 Yes Mobi-C—Zimmer Biomet 

Cobalt-chrome-molybdenum, plasma sprayed titanium, and hydroxyapatite coating Self-adjusting mobile core Teeth 2013 Yes Yes Conditionalb Maximum spatial gradient magnetic field of <970 Gauss/cm (9.7 T/m)
5, 6, and 7 Yes Abbreviations: FDA, Food and Drug Administration; MRI, magnetic resonance imaging.
↵a MRI conditional are devices that are MRI safe under a very specific set of conditions/MRI settings provided in the labeling.
↵b Patients can safely undergo magnetic resonance (MR) scanning based on the following MR specifications established through nonclinical testing: (1) static magnetic field of 1.5 and 3.0 Tesla only, (2) specified maximum spatial gradient magnetic field (implant specific), and (3) maximum MR system reported, whole body averaged specific absorption rate of 2 W/kg in normal operating mode.
Author (y) Study Treatment Follow-Up (mo) Number of Levels Radcliff et al (2017)9 Mobi-C 84 1 Vaccaro et al (2018)18 Secure-C 84 1 Garrido et al (2010)19 Bryan 48 1 Burkus et al (2014)20 Prestige ST 48 1 Rožanković et al (2014)21 Discover 24 1 Hisey et al (2016)22 Mobi-C 60 1 Janssen et al (2015)24 ProDisc-C 84 1 Phillips et al (2015)23 Porous Coated Motion (PCM) 60 and 84 1 Sasso et al (2017)26 Bryan 84 and 120 1 Sasso et al (2007)25 Bryan 24 1 Skeppholm et al (2015)10 Discover 24 1 Lavelle et al (2019)27 Bryan artificial disc 120 1 Vleggeert-Lankamp et al (2019)28 ActivC 24 1 Zhang et al (2012)29 Bryan 24 1 Zhang et al (2014)30 Mobi-C 48 1 Coric et al (2018)31 Kineflex C 60 1 Coric et al (2006)32 Bryan 24 1 Donk et al (2017)33 Bryan 60 1 Cheng et al (2011)34 Bryan 36 1, 2, and 3 Porchet et al (2004)35 Prestige II 24 1 Miller et al (2008)36 Bryan 84 1 McAfee et al (2010)37 PCM 24 1 Nabhan et al (2007)39 ProDisc-C 36 1 Nabhan et al. (2007)39 ProDisc-C 6 1 Hou et al (2016)40 Mobi-C 60 1 Riina et al (2008)41 Prestige ST 24 1 Sundseth et al (2017)42 Discover 24 1 Hacker (2005)43 Bryan 12 1 Skeppholm et al (2013)44 Discover 24 1 MacDowall et al (2019)45 Discover 60 1 Radcliff et al (2017)9 Mobi-C 84 2 Skeppholm (2015)10 Discover 24 2 Cheng et al (2009)48 Bryan 24 2 Yang et al (2018)47 Mobi-C 81 2 Author (y) Sample Size Patient-Reported Outcomes Secondary Surgery ASD at Follow-Up Conclusions Radcliff et al (2017)9 N = 245 Intervention n = 164 NDI recovery ratio: 67%
VAS neck pain recovery ratio: 71%
VAS arm pain recovery ratio: 73%
SF-12 PCS recovery ratio: 22%
SF-12 MCS recovery ratio: 11%
NDI status at follow-up: 84.6% improved, 14.2% not improved, and 1.2% worse
Patient satisfaction: 90.9%a
VAS neck pain status at follow-up: 87.5% improved, 8.8% not improved, and 3.8% worse3% 40.4% (superior level) and 43.8% (inferior level)a The intervention provided a similar reduction in patient-reported outcomes of pain and function while providing a lower risk for reoperation at both treated and adjacent levels. Control n = 81 NDI recovery ratio: 64%
VAS neck pain recovery ratio: 71%
VAS arm pain recovery ratio: 63%
SF-12 PCS recovery ratio: 17%
SF-12 MCS recovery ratio: 13%
NDI status at follow-up: 84.8% improved, 12.7% not improved, and 2.5% worse
Patient satisfaction: 77.8%
VAS neck pain status at follow-up: 83.3% improved, 8.8% not improved, and 1.3% worse12.3% 65.1% (superior level) and 63% (inferior level) Vaccaro et al (2018)18 N = 225 Intervention n = 124 NDI improvement >25%: 90.4%
NDI improvement >15%: 88.8%
VAS neck pain success: 85.7%
VAS arm pain success, left: 85.7%
VAS arm pain success, right: 84.9%
SF-36 PCS success: 72%
SF-36 MCS success: 47.2%
Neurological status stable/improved: 94.2%
Patient satisfaction: 96%a4.2% 17% (symptoms attributable to adjacent level disease) Intervention was noninferior to control in terms of providing long-term pain relief and functional improvement in patients diagnosed with single-level cervical degenerative disc refractory to nonoperative treatment.
Intervention statistically superior to control in terms of composite overall success and patient satisfaction.
Intervention had lower rates of secondary surgery (index and adjacent levels).
Control n = 101 NDI improvement >25%: 86%
NDI improvement >15%: 84.1%
VAS neck pain success: 78.3%
VAS arm pain success, left: 75.5%
VAS arm pain success, right: 72.6%
SF-36 PCS success: 74.5%
SF-36 MCS success: 43.4%
Neurological status stable/improved: 87.1%
Patient satisfaction: 88.8%15.3% 37.5% (symptoms attributable to adjacent level disease) Garrido et al (2010)19 N = 47 Intervention n = 21 NDI Success: 93.3%
Neck pain score % improvement: 80%
Arm pain score % improvement: 86%
SF-36 PCS score % improvement: 50%
SF-36 MCS score % improvement: 24%4.7% 5% (secondary surgery due to adjacent level disease) Although not statistically significant, there appear to be clinically favorable outcomes regarding functional outcomes and adjacent segment disease for the arthroplasty cohort. Control n = 26 NDI success: 82.4%
Neck pain score % improvement: 67%
Arm pain score % improvement: 73%
SF-36 PCS score % improvement: 50%
SF-36 MCS score % improvement: 13%23% 12% (secondary surgery due to adjacent level disease) Burkus et al (2014)20 N = 395 Intervention n = 212 NDI Success: 83.4%
Arm pain improvement: 46.4 points
Neck pain improvement: 55.1 points
SF-36 PCS scores: 45.1 points at final follow-up
Neurological success: 88.2%a4.8% 4.6% (secondary surgery at adjacent levels) Intervention has the potential for preserving motion at the operated level while providing mechanical stability and global neck mobility and pay result in a reduction in adjacent segment degeneration. Control n = 183 NDI Success: 80.1%
Arm pain improvement: 47.4 points
Neck pain improvement: 49.9 points
SF-36 PCS scores: 43.2 points at final follow-up
Neurological success: 79.7%13.7% 11.9% (secondary surgery at adjacent levels) Rožanković et al (2014)21 N = 101 Intervention n = 51 NDI score: 11.60 final (preop 50.90)a
VAS arm score: 1.70 final (preop 7.70)
VAS neck pain: 2.36 final (preop 7.56)a- - The intervention provided better results after a 2-y follow-up compared with control. Control n = 50 NDI score: 19.68 final (preop 51.20)
VAS arm score: 2.42 final (preop 7.66)
VAS neck pain: 3.46 final (preop 7.50)- - Hisey et al (2016)22 N = 245 Intervention n = 164 NDI, VAS (neck and arm), and SF-12 scores: statistically similar between intervention and control 4.9% and 3% 37.1% (superior level)a The intervention has the potential advantage of lower rates of reoperation and adjacent segment degeneration through 60 mo in treatment of single-level symptomatic cervical degenerative disc disease. Control n = 81 17.3% and 11.1% 54.7% (superior level) Janssen et al (2015)24 N = 152 Intervention n = 79 Score/Point Improvements
NDI: 31.87
SF-36 PF: 10.99
SF-36 role limitation due to physical health: 16.03
SF-36 role limitation due to emotional problems: 9.67
SF-36 energy/fatigue: 12.43
SF-36 emotional well-being: 7.59
SF-36 social functioning: 15.64
SF-36 bodily pain: 16.05
SF-36 general health: 0.21
SF-36 PCS: 12.24
SF-36 MCS: 8.93
VAS neck pain: 45.67
VAS arm pain: 40.72
VAS satisfaction with surgery: 85.81/100
Neurological success: 88%7%a 5.8%a (secondary surgery at adjacent level) At 7 y postoperatively, all outcomes were similar between the 2 cohorts. However, intervention was associated with a lower risk of secondary surgery at both index and adjacent vertebral levels. Control n = 73 Score/Point Improvements
NDI: 30.3
SF-36 PF: 9.89
SF-36 role limitation due to physical health: 15.24
SF-36 role limitation due to emotional problems: 8.01
SF-36 energy/fatigue: 10.21
SF-36 emotional well-being: 5.94
SF-36 social functioning: 15.02
SF-36 bodily pain: 15.94
SF-36 general health: 0.64
SF-36 PCS: 12.09
SF-36 MCS: 6.93
VAS neck pain: 42.88
VAS arm pain: 38.83
VAS satisfaction with surgery: 81.81/100
Neurological success: 89%18% 12.2% (secondary surgery at adjacent level) Phillips et al (2015)23 N = 293 Intervention n = 163 NDI success: 85%a
VAS neck pain success: 71.9%
VAS arm pain success: 80.6%
SF-36 PCS score improvement: 73.7%a
SF-36 MCS score improvement: 46.2%
Neurological success: 92.4%
Patient satisfaction: 86.9/100a8.5% Degeneration at Adjacent Levels
33.1% (superior)a and 49.2% (inferior)Compared with the control, the intervention group demonstrated equivalent or better clinical outcomes while preserving cervical motion.
Intervention had improved function, lower rates of prolonged dysphagia, greater patient satisfaction, lower incidence of adjacent level degeneration, and lower rate of secondary surgery.
Control n = 130 NDI success: 74.2%
VAS neck pain success: 75.8%
VAS arm pain success: 71.1%
SF-36 PCS score improvement: 56.7%
SF-36 MCS score improvement: 54.3%
Neurological success: 87.5%
Patient satisfaction: 78.3/10013% Degeneration at Adjacent Levels
50.9% (superior) and 51.7% (inferior)Sasso et al (2017)26 N = 42 Intervention n = 19 Mean Scores at Final Follow-up
NDI: 8.05a
VAS neck pain: 1.3
VAS arm pain: 0.849% - At the final 120 mo follow-up, both groups demonstrated sustained improvement compared with the baseline. The intervention group demonstrated greater improvement in NDI compared with the control group. The reoperation rate was lower in the intervention group, but this was not statistically significant. Control n = 23 Mean Scores at Final Follow-up
NDI: 15.48
VAS neck pain: 1.5
VAS arm pain: 0.7432% - Sasso et al (2007)25 N = 115 Intervention n = 56 Scores at Final Follow-up
NDI: 11a
Neck pain VAS: 16a
Arm pain VAS: 14a
SF-36 PCS: 51a
SF-36 MCS: 543.57% 3.57% (secondary procedure for adjacent level disease) At a 2 y follow-up, the intervention group demonstrated statistically significant improvements in NDI, neck pain, and SF-36 PCS. Control n = 59 Scores at Final Follow-up
Final NDI: 20
Neck pain VAS: 32
Arm pain VAS: 28
SF-36 PCS: 46
SF-36 MCS: 526.7% 3.39% (secondary procedure for adjacent level disease) Skeppholm et al (2015)10 N = 125 Intervention n = 67 Mean Score at Final Follow-up
NDI: 39.1
EQ-5D: 0.72
VAS neck pain: 25.6
VAS arm pain: 19.211% - No significant superiority in NDI or secondary outcome variables in the intervention group compared with the ACDF group.
Reoperations were higher in the intervention group, but not significantly so.
No differences in secondary surgery for adjacent segment disease were seen after 2 y.
Artificial disc replacement did not result in better outcomes compared with fusion measured with NDI 2 y after surgery.
Control n = 58 Mean Score at Final Follow-up
NDI: 40.1
EQ-5D: 0.71
VAS neck pain: 28.7
VAS arm pain: 20.14% - Lavelle et al (2019)27 N = 232 Intervention n = 128 Mean NDI improvement: ∆38.3a
NDI success rate: 90.5%a
Mean VAS neck pain improvement: ∆54.3
Mean VAS arm pain score: ∆58.1
SF-36 PCS score improvement: ∆14.9a9.7% 9.7% (secondary surgery at adjacent levels) While there may be some convergence of clinical benefit over time, there is maintenance of advantage in preserved motion and rates of reoperation for cervical disc arthroplasty. Control n = 104 Mean NDI improvement: ∆31.1
NDI success rate: 75.7%
Mean VAS neck pain improvement: ∆49.2
Mean VAS arm pain score: ∆51.6
SF-36 PCS score improvement: ∆12.615.8% 15.8% (secondary surgery at adjacent levels) Vleggeert-Lankamp et al (2019)28 N = 98 Intervention n = 32 Score at Final Follow-up
NDI: 20 ± 22 (preop 47 ± 17)
VAS arm pain: 17 ± 30 (preop 60 ± 24)
VAS neck pain: 23 ± 32 (preop 50 ± 27)
EQ-5D: 0.82 ± 0.23 (preop 0.59 ± 0.20)
VAS health: 74 ± 25 (preop 45 ± 22)
Likert global health recovery (% satisfied): 65.6%
Likert arm pain (% satisfied): 65.6%
SF-36 PCS: 72.2 ± 27 (preop 41.3 ± 14)
SF-36 MCS: 74.3 ± 25 (preop 54.9 ± 25)6.2% - It seems that there is no strong evidence in favor of 1 of the 3 treatment strategies based on the 2 y evaluation of results. They all give comparable clinical results, and all 3 options are acceptable. Control 1 (ACDF) n = 34 Score at Final Follow-up
NDI: 19 ± 18 (preop 41 ± 13)
VAS arm pain: 15 ± 23 (preop 57 ± 20)
VAS neck pain: 23 ± 27 (preop 53 ± 26)
EQ-5D: 0.83 ± 0.18 (preop 0.70 ± 0.18)
VAS health: 74 ± 24 (preop 53 ± 23)
Likert global health recovery (% satisfied): 67.6%
Likert arm pain (% satisfied): 73.5%
SF-36 PCS: 75.9 ± 23 (preop 44.7 ± 15)
SF-36 MCS: 81.6 ± 19 (preop 61.7 ± 22)11.8% - Control 2 (ACD) n = 32 NDI: 19 ± 15 (preop 45 ± 16)
VAS arm pain: 18 ± 25 (preop 64 ± 22)
VAS neck pain: 21 ± 23 (preop 56 ± 31)
EQ-5D: 0.83 ± 0.17 (preop 0.54 ± 0.20)
VAS health: 69 ± 24 (preop 48 ± 26)
Likert global health recovery (% satisfied): 62.5%
Likert arm pain (% satisfied): 68.8%
SF-36 PCS score: 68.3 ± 24 (preop 41.2 ± 14)
SF-36 MCS score: 71.2 ± 23 (preop 57.9 ± 21)6.2% - Zhang et al (2012)29 N = 109 - Intervention n = 56 NDI improvement: ∆36.89
VAS neck pain improvement: ∆49.27
VAS arm pain improvement: ∆54.961.8% - Baseline changes in NDI and neck and arm pain were similar in patients in the intervention and control groups. Control n = 53 NDI improvement: ∆38.98
VAS neck pain improvement: ∆47.38
VAS arm pain improvement: ∆55.457.5% - Zhang et al (2014)30 N = 111 Intervention n = 55 JOA, VAS, and NDI scores at final follow-up: Not statistically different between groups - - - Control n = 56 - - - Coric et al (2018)31 N = 269 Intervention n = 136 NDI score: 18.5 (preop 62.8)
VAS pain score: 20.8 (preop 77.1)8.8% (rate of reoperation or revision) ASD scores at final follow-up: 65.7% (superior level, preop 51.1%)a and 84.9% (inferior level, preop 47.4%) There were statistically significant differences between the groups, favoring the intervention group when evaluating ASD and some clinical outcome measures. At no point was there a significant difference favoring the control. Control n = 133 NDI score: 23 (preop 61.8)
VAS pain scores: 24.2 (preop 75.7)8.3% (rate of reoperation or revision) ASD scores at final follow-up: 93.2% (superior level, preop 53.1%) and 86.8% (inferior level, preop 53.3%) Coric et al (2006)32 N = 33 Intervention n = 17 Score at Final Follow-up
NDI: 9 (preop 41)
SF-36 PCS: 50 (preop 34)
SF-36 MCS: 56 (preop 48)
VAS arm pain: 10 (preop 60)
VAS neck pain: 18 (preop 79)- - Similar improvements in the clinical parameters were observed in both groups, but in the intervention group, there was radiographic evidence of motion at the treated level. Control n = 16 Score at Final Follow-up
NDI: 23 (preop 48)
SF-36 PCS: 46 (preop 32)
SF-36 MCS: 49 (preop 51)
VAS arm pain: 30 (preop 61)
VAS neck pain: 38 (preop 68)- - Donk et al (2017)33 N = 140 All Groups at Final Follow-up
NRS arm pain: 1.8 ± 2.5
NRS neck pain: 1.9 ± 2.6Intervention n = 49 Mean Improvement at Final Follow-up
NDI: 7.5 ± 8.5 (preop 18.8 ± 7.5)
SF-36 PCS: 32.1 ± 2.5 (preop 44.1 ± 13.9)
SF-36 MCS: 22.8 ± 2.1 (preop 58.3 ± 22.2)2%a 0% (surgery for ASD) This trial did not detect a difference between 3 surgical modalities for treating a single-level degenerative disc disease. There was also no statistically significant difference between groups regarding surgery for adjacent segment disease. Control 1 (ACDF) n = 46 Mean Improvement at Final Follow-up
NDI: 7.5 ± 8.5 (preop 18.8 ± 7.4)
SF-36 PCS: 32.1 ± 2.5 (preop 44.0 ± 11.0)
SF-36 MCS: 22.8 ± 2.1 (preop 55.7 ± 21.1)13%a 10.6% (surgery for ASD) Control 2 (ACD) n = 45 Mean Improvement at Final Follow-up
NDI: 7.5 ± 8.5 (preop 17.1 ± 6.4)
SF-36 PCS: 32.1 ± 43.6
SF-36 MCS: 22.8 ± 2.1 (preop 62.1 ± 18.8)8.9%a 6.7% (surgery for ASD) Cheng et al (2011)34 N = 83 Both Groups at Final Follow-up
NDI, SF-36, and JOA scores: Patients in intervention group had significantly betterIntervention n = 41 Modified Odom’s Criteria score at final follow-up: 58.5% excellent, 34.1% good, and 7.3% fair - - Intervention is safe for the treatment of patients with cervical myelopathy and comparable to control in improving functional outcomes at 1 and up to 3 y after surgery. Control n = 42 Modified Odom’s Criteria score at final follow-up: 58.5% excellent, 25% good, 15% fair, and 5% poor - - Porchet et al (2004)35 N = 55 Intervention n = 27 NDI and arm pain frequency and intensity at final follow-up: Improvement seen was statistically equivalent between both groups
Neck pain frequency and intensity:
Statistical equivalence could not be shown between the 2 groups
SF-36 at final follow-up: Differences in scores between treatment groups were not statistically significant0% 0% Most outcomes measured seemed to favor the intervention group, but the differences were not statistically superior.
Radiographic analyses showed that the intervention maintained motion at the treated level without actual adjacent segment compromise.Control n = 28 7.47% (adjacent level secondary surgery due to secondary myelopathy) Miller et al (2018)36 N = 70 Intervention n = 34 - - Adjacent level degeneration: 0.318 (preop 0.313) at 84 mo; 0.295 (preop 0.313) at 60 mo Adjacent level degeneration occurred in a similar manner in both the intervention and control groups. Control n = 36 - - Adjacent level degeneration: 0.299 (preop 0.310) at 84 mo; 0.310 (preop 0.310) at 60 mo McAfee et al (2010)37 N = 251 Intervention n = 151 Incidence at Final Follow-up
Dysphagia: 85% none, 11.9% mild, 2.9% moderate, and 0% severea
Dysphonia: 9.0 ± 15.4- - In this study, the incidence of postoperative dysphagia and the long-term resolution of dysphagia were greatly improved in the intervention group compared with the control group. Control n = 100 Incidence at Final Follow-up
Dysphagia: 72.4% none, 13.8% mild, 13.8% moderate, and 0% severe
Dysphonia: 13.1 ± 18.8- - Nabhan et al (2007)38 N = 41 Intervention n = 20 VAS neck pain: 1.7 (preop 6.0)
VAS arm pain: 1.2 (preop 7.3)- - After both procedures, a significant pain reduction in neck and arm was observed, with no significant differences between both groups. Control n = 21 VAS neck pain: 2.5 (preop 6.2)
VAS arm pain: 1.7 (preop 7.2)- - Nabhan et al., 200739 N = 33 Intervention n = 16 VAS neck pain: 2.8 (preop 6.2)
VAS arm pain: 1.4 (preop 7.6)- - Both treatments resulted in significant reduction of neck and arm pain without statistical difference between groups Control n = 17 VAS neck pain: 2.0 (preop 6.4)
VAS arm pain: 1.7 (preop 7.2)- - Hou et al (2016)40 N = 99 Intervention n = 51 JOA score: 14.7
VAS for pain scores: 0.4
NDI scores: 19.71.97% - Both intervention and control treatments are effective in improving clinical status at up to 5 y follow-up. Intervention is a safe and encouraging alternative to the control treatment, particularly in patients with single-level cervical disc degeneration who require surgery. Control n = 48 JOA score: 14.5
VAS for pain scores: 0.4
NDI scores at final follow-up: 18.514.6% - Riina et al (2008)41 N = 16 - - Intervention n = 9 Improvement at Final Follow-up
VAS neck pain: 17.9 (preop 74.8)
VAS arm pain: 17.2 (preop 69.1)
NDI: 18.9 (preop 65.5)
Neurological status: 100% motor function and reflexes, 77.8% sensory function, and overall
SF-36 PCS success rate: 77.8%
SF-36 MCS success rate: 66.7%Neurological function and neck pain were better addressed in the intervention group, but arm pain was better addressed in the control group. The intervention performed as least as well as the control. Control n = 7 Improvement at Final Follow-up
VAS neck pain: 17.4 (preop 71.6)
VAS arm pain: 8.6 (preop 72.7)
NDI: 22.3 (preop 60.2)
Neurological status: 100% motor, 85.7% sensory and reflexes, and 71.4% overall
SF-36 PCS success rate: 100%
SF-36 MCS success rate: 57.1%Sundseth et al (2017)42 N = 120 Intervention n = 60 Improvement at Final Follow-up
NDI: 25 (preop 45.7)
EQ-5D-3L: 0.72 (preop 0.37)
SF-36 PCS: 46.4 (preop 32.9)
SF-36 MCS: 52.3 (preop 47.4)
NRS 11th arm pain: 2.0 (preop 6.0)
NRS 11th neck pain: 3.0 (preop 7.0)13.3% (reoperations at index level) - Intervention treatment was not superior to control treatment regarding clinical outcomes. The rate of index level reoperations was significantly higher, and the duration of the surgical procedure was longer with the intervention treatment. Control n = 60 Improvement at Final Follow-up
NDI: 21.2 (preop 51.2)
EQ-5D-3L: 0.72 (preop 0.28)
SF-36 PCS: 46.9 (34.9)
SF-36 MCS: 50.3 (preop 44.2)
NRS 11th arm pain: 1.5 (preop 6.5)
NRS 11th neck pain: 3.0 (preop 7.0)1.67%a (reoperations at index level) - Hacker (2005)43 N = 28 - - Intervention n = 13 NDL, neck pain, arm pain, SF-36 PCS, and SF-36 MCS: No significant difference between groups - - Preoperative symptoms improved more in intervention group than in control group, but the difference was not statistically significant. Control n = 15 - - Skeppholm et al (2013)44 N = 136 Intervention n = 76 Median dysphagia symptom questionnaire (DSQ) level at final follow-up: 0a - - Prolonged postoperative dysphagia could be explained by factors such as the bulk of implants and decreased motion of the cervical spine. Control n = 60 Median DSQ level at final follow-up: 1 - - MacDowall et al (2019)45 N = 137 Intervention n = 67 Improvement at Final Follow-up
NDI: 36 (preop 64)
EQ-5D: 0.62 (preop 0.37)
EQ-5D health: 67.3 (preop 47.2)
VAS neck pain: 29.1 (preop 47.2)
VAS arm pain: 24 (preop 57)
DSQ level: 1.6 (preop 1.4)25.4% 7.46% (secondary surgery due to clinical adjacent segment pathology at final follow-up)
24% (incidence of mild clinical adjacent segment pathology at final follow-up)At 5 y, patients in the intervention group did not have better clinical or radiographic outcomes compared with the control group. However, the intervention group had a significantly lower mean DSQ score than the control group at the final follow-up. Control n = 70 Improvement at Final Follow-up
NDI: 32.2 (preop 61)
EQ-5D: 0.72 (preop 0.46)
EQ-5D health: 70.1 (preop 44)
VAS neck pain: 31.8 (preop 58.6)
VAS arm pain: 23.8 (preop 56.7)
DSQ level: 2.3 (preop 1.4)10% 7.41% (secondary surgery due to clinical adjacent segment pathology at final follow-up)
20% (incidence of mild clinical adjacent segment pathology at final follow-up)Phillips et al (2021)23 N = 316 Intervention n = 152 - 1.9% Did not assess - Control n = 164 - 4.8% Did not assess - Radcliff et al (2017)9 N = 330 Intervention n = 225 Improvement at Final Follow-up
NDI: 18.0 ± 19.1 (preop 53.8 ± 15.4)a
VAS neck pain: 19.0 ± 27.1 (preop 71.2 ± 20.5)
VAS arm pain: 15.9 ± 25.7 (preop 68.8 ± 25.0)
SF-12 PCS: 46.3 ± 11.1 (preop 33.4 ± 6.7)
SF-12 MCS: 52.0 ± 10.1 (preop 41.9 ± 11.3)
NDI and pain status: 80.8% improved, 16.5% not improved, and 2.7% worse4.4% (index level)a and 4.4% (adjacent level)a Adjacent Level Degeneration
37.5% (superior level) and 30.3% (inferior level)The intervention provided a similar reduction in patient-reported outcomes of pain and function while providing a lower risk for reoperation at both treated and adjacent levels. The difference in clinical effectiveness of intervention vs control becomes more apparent as treatment increases from 1 to 2 levels, indicating a significant benefit for intervention treatment over control treatment for 2-level procedures. Control n = 105 Improvement at Final Follow-up
NDI: 26.2 ± 22.4 (preop 55.7 ± 15.2)
VAS neck pain: 28.7 ± 30.4 (preop 75.1 ± 18.9)
VAS arm pain: 18.4 ± 27.0 (preop 73.1 ± 21.9)
SF-12 PCS: 43.7 ± 11.9 (preop 32.5 ± 7.7)
SF-12 MCS: 49.1 ± 12.7 (preop 42.0 ± 12.0)
NDI and pain status: 70.2% improved, 25.9% not improved, and 3.8% worse10.5% (index level) and 11.4% (adjacent level) Adjacent Level Degeneration
80.8% (superior level) and 66.7% (inferior level)Skeppholm (2015)10 N = 125 Intervention n = 67 - 11% - - Control n = 58 - 4% - - Cheng et al (2009)46 N = 62 Intervention n = 30 Improvement at Final Follow-up
VAS neck pain: 1.5 (preop 7.3)a
VAS arm pain: 1.4 (preop 7.1)a
NDI: 11 (preop 50)a
SF-36 PCS: 50 (preop 35)a- - Intervention treatment was shown to be reliable and safe for the treatment of patients with 2-level cervical disc disease. Control n = 32 Improvement at Final Follow-up
VAS neck pain: 2.6 (preop 7.1)
VAS arm pain: 2.7 (preop 7.2)
NDI: 19 (preop 51)
SF-36 PCS: 45 (preop 34)- - Yang et al (2018)47 N = 80 Intervention n = 38 Improvement at Final Follow-up
NDI: Scores at final follow-up were significantly higher in the control group than intervention group
JOA: Scores at final follow-up were statistically similar between groups
VAS: Scores were significantly lower in the intervention group than in the control group0% Adjacent Segment Degeneration
15.7% (superior level)a and 7.8% (inferior level)aIntervention treatment was safe and effective and a statistically superior alternative to ACDF for degenerative disc disease at 2 contiguous levels.
Intervention treatment could reduce the occurrence of ASD at the superior and inferior adjacent segments by reducing the ROM.Control n = 42 0% Adjacent Segment Degeneration
45.7% (superior level) and 33.35% (inferior level)Abbreviations: ACDF, anterior cervical discectomy and fusion; ASD, adjacent segment disease; JOA, Japanese Orthopaedic Association ; NDI, Neck Disability Index; preop, preoperative; ROM, range of motion; SF-36, short form-36; SF-12 MCS, short form-12 mental component score; SF-36 MCS, short form 36-mental component score; SF-12 PCS, short form-12 physical component score; SF-36 PCS, short form-36 physical component score; VAS, visual analog scale.
↵a Findings were based on sample sizes that varied from the original cohort due to loss of follow-up (attrition rates <5%).
Indications 1. Skeletally mature patients 2. Reconstruction of the disc from C3 to C7 following discectomy 3. Single or 2 contiguous levels 4. Intractable radiculopathy (with or without neck pain) or myelopathy (due to abnormality at the level of the disc space) 5. At least 1 of the following confirmed by imaging (computed tomography, magnetic resonance imaging, or x-rays): Herniated nucleus pulposus
Spondylosis (defined by the presence of osteophytes)
Visible loss of disc height compare towith adjacent levels
6. Failed 6 wk of conservative management or progressive signs or symptoms despite nonoperative treatment Contraindications 1. Acute or chronic infection (systemic or at the operative site) 2. Osteoporosis or osteopenia (defined as DEXA bone density measured T-score < −2.5 or <1.5, respectively) 3. Known allergy or sensitivity to implant materials (cobalt, chromium, molybdenum, titanium, hydroxyapatite, or polyethylene) 4. Compromised vertebral bodies at the index level(s) due to previous trauma to the cervical spine or significant cervical anatomical deformity or disease (eg, ankylosing spondylitis and rheumatoid arthritis) 5. Marked cervical instability on resting lateral or flexion/extension radiographs (demonstrated by translation <3.5 mm and/or >11° angular difference to that of either level adjacent to the treated level(s)) 6. Severe facet joint disease or degeneration 7. Severe spondylosis (defined as bridging osteophytes, loss of disc height >50%, or <2° of motion), as this may lead to limited range of motion and may encourage bone formation (eg, heterotopic ossification and fusion) Abbreviation: DEXA, dual-energy x-ray absorptiometry.
a Derived from Summary of Safety and Effectiveness Data for the ProDisc Total Disc Replacement and Mobi-C Cervical Disc Prosthesis.
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.