


Abstract
Background Effective 1 January 2017, single-level endoscopic lumbar discectomy received a Category I Current Procedural Terminology (CPT) code 62380. However, no work relative value units (RVUs) are currently assigned to the procedure. An international team of endoscopic spine surgeons conducted a study, endorsed by several spine societies, analyzing the learning curve, difficulty, psychological intensity, and estimated work RVUs of endoscopic lumbar spinal decompression compared with other common lumbar spine surgeries.
Methods A survey comparing CPT 62380 to 10 other comparator CPT codes reflective of common spine surgeries was developed to assess the work RVUs in terms of learning curve, difficulty, psychological intensity, and work effort using a paired Rasch method.
Results The survey was sent to 542 spine specialists. Of 322 respondents, 150 completed the survey for a 43.1% completion rate. Rasch analysis of the submitted responses statistically corroborated common knowledge that the learning curve with lumbar endoscopic spinal surgery is steeper and more complex than with traditional translaminar lumbar decompression surgeries. It also showed that the psychological stress and mental and work effort with the lumbar endoscopic decompression surgery were perceived to be higher by responding spine surgeons compared with posterior comparator decompression and fusion surgeries and even posterior interbody and posterolateral fusion surgeries. The regression analysis of work effort vs procedural difficulty showed the real-world evaluation of the lumbar endoscopic decompression surgery described in CPT code 62380 with a calculated work RVU of 18.2464.
Conclusion The Rasch analysis suggested the valuation for the endoscopic lumbar decompression surgery should be higher than for standard lumbar surgeries: 111.1% of the laminectomy with exploration and/or decompression of spinal cord and/or cauda equina (CPT 63005), 118.71% of the laminectomy code (CPT 63047), which includes foraminotomy and facetectomy, 152.1% of the hemilaminectomy code (CPT 63030), and 259.55% of the interlaminar or interspinous process stabilization/distraction without decompression code (CPT 22869). This research methodology was endorsed by the Interamerican Society for Minimally Invasive Spine Surgery (SICCMI), the Mexican Society of Spinal Surgeons (AMCICO), the International Society For Minimally Invasive Spine Surgery (ISMISS), the Brazilian Spine Society (SBC), the Society for Minimally Invasive Spine Surgery (SMISS), the Korean Minimally Invasive Spine Surgery (KOMISS), and the International Society for the Advancement of Spine Surgery (ISASS).
Clinical Relevance This study provides an updated reimbursement recommendation for endoscopic spine surgery.
Level of Evidence Level 3.
- CPT® code 62380
- RUC
- Rasch methodology
- endoscopic surgery
- learning curve
- difficulty
- psychological stress
- work effort
Introduction
On 1 January 2017, a new Category I Current Procedural Terminology (CPT) code, 62380, was introduced. This code outlines procedures involving “Endoscopic, percutaneous, or minimally invasive interventions (utilizing direct visualization) complemented with image guidance. Specifically, it covers endoscopic decompression of the spinal cord, nerve root(s), including laminotomy, partial facetectomy, foraminotomy, discectomy, and/or resection of herniated intervertebral disc at a singular interspace within the lumbar region.”1 The diagnostic protocol for identifying the primary cause of lumbar pain was recently published in a contemporary scholarly article, which gained endorsement from 14 global spine surgeon societies.2,3 These prestigious bodies include the Inter-American Society For Minimally Invasive Spine Surgery–La Sociedad Interamericana De Cirugía De Columna Mínimamente Invasiva (SICCMI), the Spine Division of the Society For Brain Mapping and Therapeutics, the International Society for Minimal Intervention in Spinal Surgery (ISMISS), the Korean Minimally Invasive Spine Society (KOMISS), the Minimally Invasive Surgery Section of the Chinese Orthopedic Association (COA-MIS SECTION), The Colombian Spine Society, the Bolivian Spine Association, the Iberolatinoamerican Spine Society – La Sociedad Iberolatinoamericana De Columna (SILACO), the Mexican Association of Spinal Surgeons – Associacion Mexicana De Cirujanos De Columna (AMCICO), the Federation of Latinamerican Neurosurgical Societies–Federación Latino-Americana De Sociedades De Neurocirugía (FLANC), the Latin American Society of Neurosurgeons of USA and Canada, the Brazilian Spine Society–Sociedade Brasiliera De Columna (SBC), the Brazilian Society For Thoracic Surgery - Sociedade Brasileira de Cirurgia Torácica, and the International Intradiscal Therapy Society.
However, as of now, the American Medical Association’s (AMA) Specialty Society Relative Value Scale Update Committee (RUC) has not recommended to the Centers for Medicare and Medicaid Services (CMS) any work relative value units (RVUs) for CPT code 62380. Consequently, this study was conducted to objectively measure the learning curve effort required to attain the necessary skills for performing endoscopic lumbar decompression, along with assessing its psychological intensity, stress on the surgeon, and associated work effort. This assessment aimed to compare these aspects with other commonly performed lumbar spinal surgeries based on the feedback from spine surgeons experienced in these procedures. For this purpose, the authors surveyed more than 500 surgeons employing a clinical vignette of a typical patient with lumbar spine disease causing sciatica-type back and leg pain employing the Rasch methodology.
Developed by a Danish mathematician Dr. Georg William Rasch, the Rasch model is a psychometric tool to analyze categorical data, such a questionnaire responses. It evaluates these responses based on the balance between the respondent’s abilities, attitudes, or personality traits and the item’s difficulty. This model has diverse applications, from marketing to health economics.4 A neurosurgeon, Dr. Robert A. Florin, who served on the RUC for many years, utilized the methodology to find the relative work effort of health care procedures. The Rasch model employed in this study utilized paired comparisons of CPT codes, where respondents indicated which procedure in each pair required more effort. Subsequently, logistic regression methods estimated the probability of each procedure being more challenging, intense, or laborious, providing a difficulty, intensity, and work effort score for each procedure. After generating these scores, RVUs were estimated through regression analysis using existing RVUs. The ISASS Coding and Reimbursement Task Force has also employed this methodology5–7 for refinement to either rectify undervalued CPT Category I codes or to recommend interim RVUs for new CPT Category III codes to prevent underutilization of new technologies or procedures.
The present study’s objective was to facilitate discussion regarding the appropriate valuation of modern lumbar endoscopic decompression surgery. This procedure often extends beyond a simple discectomy described under CPT code 62380 and involves many additional steps to address bony and soft tissue stenosis, instability, and deformity of the diseased lumbar motion segment. The study aimed to ensure accurate valuation of this complex surgery, fostering alignment between the AMA’s RUC and CMS to prevent misvaluation in the future.
Methods
Surgeon Survey
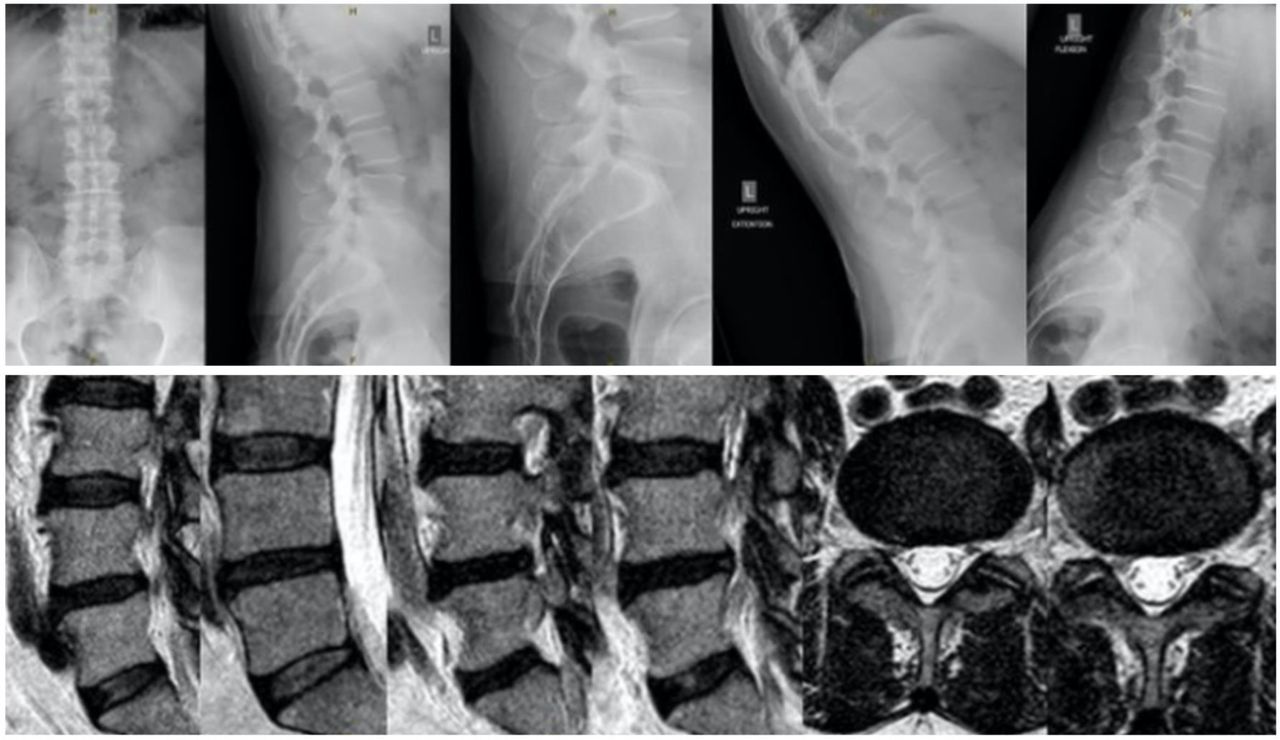
The authors conducted an extensive online survey targeting 542 surgeons via www.typeform.com utilizing email, chat groups, and messaging platforms like WhatsApp for distribution. This survey revolved around a clinical case (Figure 1) of a patient with persistent sciatica-type leg pain, without back discomfort, due to neurogenic claudication. The objective was to collect insights from surgeons regarding the learning curve, mental demand, and workload of the endoscopic lumbar decompression procedure in relation to other prevalent lumbar surgeries. Additionally, the survey included questions about the practice environment, postgraduate education, and experience with endoscopic procedures. The survey spanned from 22 September 2023 to 28 September 2023. After the survey completion, the data were exported to Excel and then analyzed using IBM SPSS (version 27) and Jamovi (version 2.3) software. The analysis employed descriptive statistics to quantify responses, calculate averages, ranges, deviation, and percentages. The χ 2 test was applied to assess the correlation between variables. Incomplete answers factored into the percentage analysis and topped each data chart. A P value below 0.05 was deemed significant, and a 95% confidence interval was applied to all statistical evaluations.

A 67-year-old man with an L4/L5 spinal stenosis causing right leg pain due to neurogenic claudication without back pain. Conservative treatments have been exhausted and failed. Imaging demonstrates foraminal and lateral spinal stenosis. An endoscopic decompression of L4/L5 foramen and the lateral canal is contemplated with the endoscopic technique of your choice.
The Rasch Methodology
The Rasch model is a part of item response theory (IRT) used to analyze categorical data, often from assessments or questionnaires. Only input data from surgeons performing the lumbar endoscopic decompression procedures were included in the “dichotomous Rasch analysis,” with 2 possible outcomes. In a dichotomous Rasch model, the probability of a specific outcome (eg, answering a question correctly) is modeled as a function of both the ability of the person (“respondent”) and the difficulty of the item. The fundamental premise of the Rasch model is that the probability of a successful outcome increases as the person’s ability increases or as the item difficulty decreases. In the context of the learning curve associated with lumbar endoscopic surgery and its mental and work effort assessments, outcomes responses selected for the dichotomous Rasch analysis were “easier” or “harder” where the procedural description of a CPT code of traditional spine surgeries (Table 1) was paired with the work described by the lumbar endoscopic decompression CPT code 62380. Eleven comparator CPT codes were employed (Table 1). Two additional responses were possible: Responding surgeons could indicate that endoscopy has an equal learning curve or that they were not performing the procedure paired with endoscopy. In the latter case, their response was not included in the dichotomous analysis.
CPT codes representative of 2023 work RVUs.
To follow the dichotomous Rasch methodology and to avoid misvaluation of the learning curve and mental or work effort associated with the lumbar endoscopic decompression, surgeons’ responses indicating that the paired spinal surgery had “Equal” effort were recoded as “Harder” since they were not associated with less effort than the paired spinal surgery. The advantage of the dichotomous Rasch model is that it allows one to place surgeons and surgery types on the same linear scale. Florin successfully employed this dichotomized analysis model to find the relative work effort of neurosurgical procedures.9 In mathematical terms, the dichotomous Rasch model represents the log odds (or logit) of a person successfully responding to an item as the difference between the person’s ability and the item’s difficulty. This model employs χ 2 fit statistics to control the applicability of data to the model. The χ 2 in common use is known as outfit and infit. These are reported as mean squares, χ 2 statistics divided by their degrees of freedom so that they have a ratio-scale form with expectation 1 and range 0 to + ∞. Outfit is based on the conventional sum of squared standardized residuals, where X is an observation, E is its expected value based on Rasch parameter estimates, and σ² is its modeled variance about its expectation. Then the squared standardized residual is


where N is the number of observations summed. In comparison, infit is an information-weighted sum. The statistical information in a Rasch observation is its variance, σ². This is larger for targeted observations and smaller for extreme observations, for example, easy items administered to able persons. Infit is

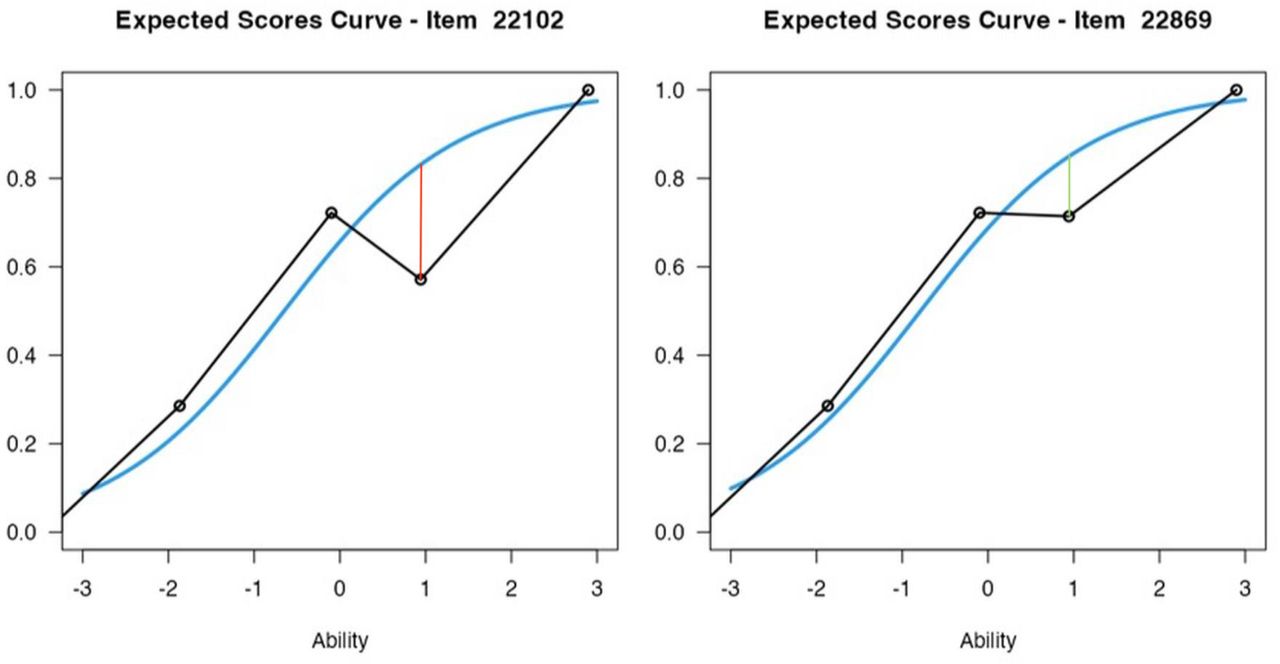
summed over the relevant observations. Fit statistics are formulated to test particular hypotheses. Outfit is dominated by unexpected outlying, off-target, low information responses and so is outlier-sensitive. Unexpected inlying patterns among informative, on-target observations dominate inlier-sensitive infit. The mean square fit statistics show the size of the randomness, that is, the amount of distortion of the measurement system. Mean squares are always positive, and 1.0 is their expected value. Values less than 1.0 indicate that observations are too predictable (redundancy, data overfit the model). Values greater than 1.0 indicate unpredictability (unmodeled noise, data underfit the model). Statistically, mean squares are χ 2 statistics divided by their degrees of freedom. Two examples of outlier-sensitive means statistics (outfit analysis) based on the conventional sum of squared standardized residuals, which is more sensitive to unexpected observations, are given in Figure 2. Surgeon responses on the difficulty of CPT 22102 compared with the lumbar endoscopy procedure showed a greater outfit from the model predicted by the Rasch analysis (indicated by the red vertical line) than for CPT code 22869 (green vertical line), thereby suggesting the presence of confounding factors affecting responses on item for CPT 22102. Infit (not shown in this graph) and outfit data between 0.6 and 1.4 indicate a good fit of the Rasch model. Outside these parameters, confounding factors are likely.

Two examples of outlier-sensitive means statistics (outfit analysis) based on the conventional sum of squared standardized residuals, which is more sensitive to unexpected observations, are shown. Surgeon responses on the difficulty of Current Procedural Terminology (CPT) code 22102 compared with the lumbar endoscopy procedure showed a greater outfit from the model predicted by the Rasch analysis (indicated by the red vertical line) than for CPT code 22869 (green vertical line), thereby suggesting the presence of confounding factors affecting responses on item for CPT code 22102. Infit (not shown in this graph) and outfit data between 0.6 and 1.4 indicate a good fit of the Rasch model. Outside these parameters, confounding factors are likely.
Work-Related RVU Regression Analysis
The Rasch analysis was executed using Jamovi (version 2.3) software and estimated the difficulty/work effort scores. According to the method of Florin,9 the scores of the accepted CPT codes were then regressed on their RVUs to generate a regression line. The line provided the best-fit estimate of the RVUs per score point (ie, the slope of the line). Then, the RVUs for CPT code 62380 were estimated by finding the RVUs that coincided with a score of 0, which was the score assigned to CPT code 62380. The simple linear regression analysis and graphics were generated by IBM SPSS (version 27).
Results
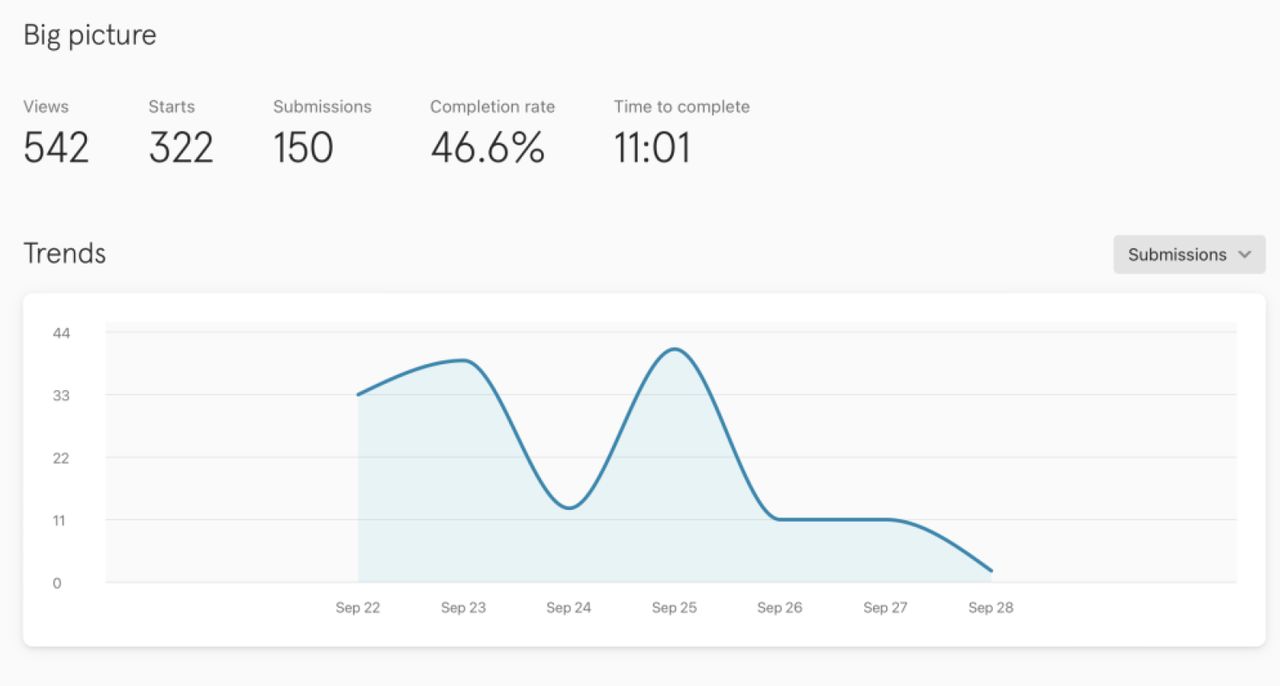
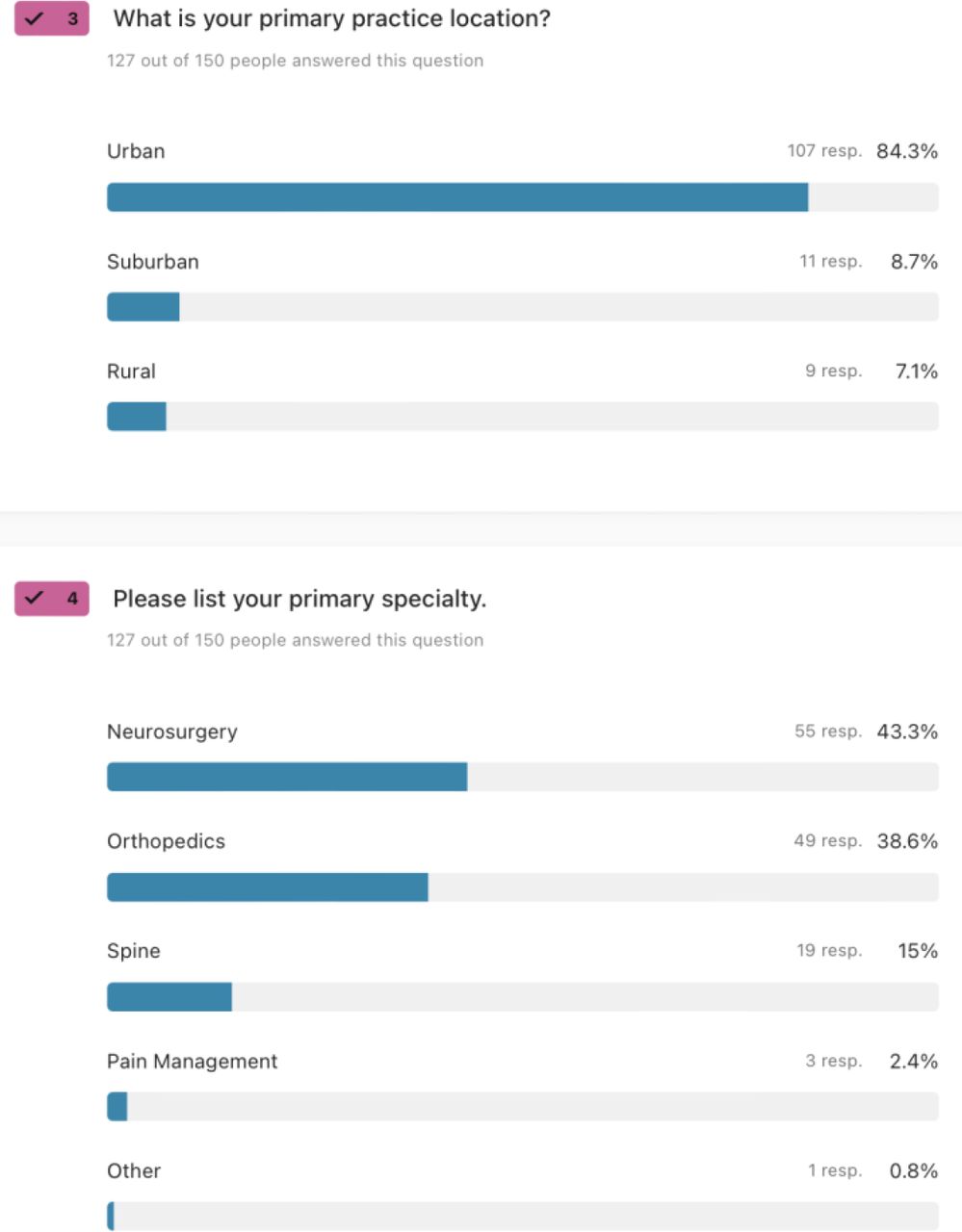
A digital questionnaire designed to objectively gauge the steepness of the learning curve, the surgeon’s psychological burden, and the laboriousness of executing endoscopic lumbar decompression relative to other prevalent lumbar spinal surgeries was accessed by 542 spine specialists. Of these, 322 embarked on the survey, with 150 providing complete, valid inputs—a completion rate of 43.1% (Figure 3). The array of respondents predominantly comprised neurosurgeons (43.3%) and orthopedic specialists (38.6%). Another 15% were exclusively devoted to spinal surgeries. A meager 2.4% of respondents practiced in pain management, ensuring that 96.9% had surgical postgraduate training. Urban clinical settings were the workplace for 84.3% of the surgeons, whereas 8.7% practiced in suburban locales, with the remaining 7.1% serving in rural environments (Figure 4).

Five hundred forty-two spine surgeons accessed the online survey aimed to obtain objective measures of the learning curve effort to obtain adequate skill level to perform the endoscopic lumbar decompression operation, its psychological intensity and stress on the surgeon, and its associated work effort in comparison to other commonly performed lumbar spinal surgeries based on the input of spine surgeons who perform these procedures. Three hundred twenty-two surgeons started the survey, and 150 submitted a valid survey recording, yielding a completion rate of 43.1%.

The majority of responding spine surgeons were neurosurgeons (43.3%). Orthopedic surgeons comprised 38.6% of the respondents, followed by 15% of surgeons who dedicated their practice entirely to the spine. Only 2.4% of the response came from pain management physicians. Therefore, 96.9% of respondents had a postgraduate education in a surgical specialty. Of the 150 responding surgeons, 84.3% worked in an urban practice setting, 8.7% worked in a suburban environment, followed by 7.1% who worked in a rural area.
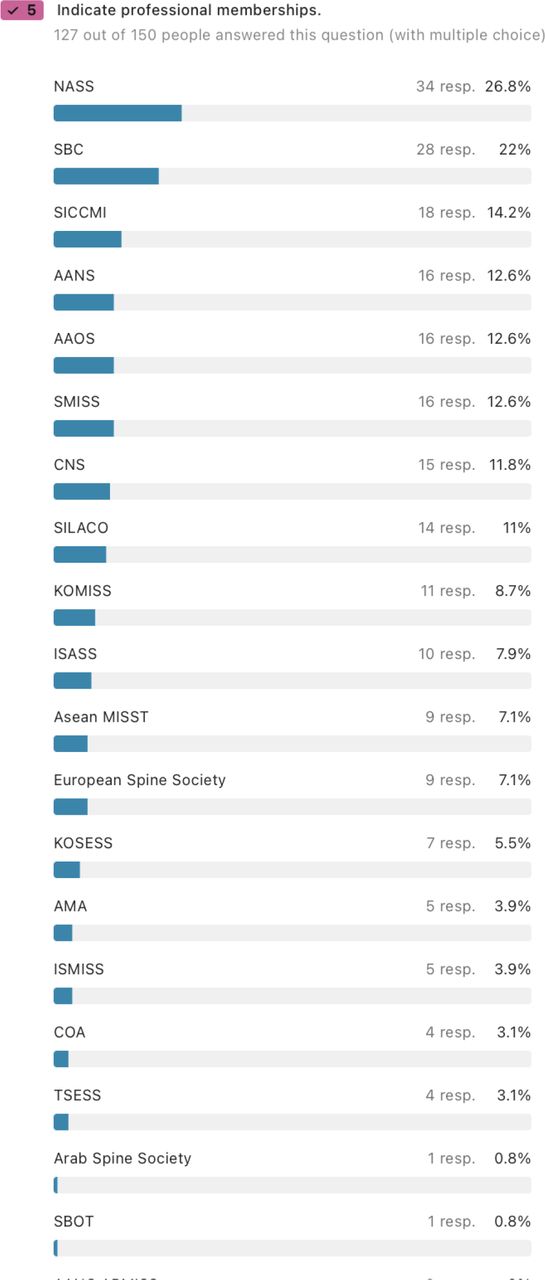
In terms of professional affiliations (Figure 5), the roster included esteemed memberships from the North American Spine Society (26.8%), SBC (22%), SICCMI (14.2%), American Association of Neurological Surgeons (12.6%), American Academy of Orthopedic Surgeons (12.6%), Society for Minimally Invasive Spine Surgery (SMISS; 12.6%), and others including Congress of Neurological Surgeons (CNS; 11.8%), SILACO (11.0%), KOMISS (8.7%), the European Spine Society (7.1%), and the International Society for the Advancement of Spine Surgery (ISASS; 7.9%). Others included the Korean Endoscopic Spine Society (5.5%), KOMISS (8.7%) AMA (3.9%), International Society for Minimal Intervention in Spinal Surgery (3.9%), Chinese Orthopedic Association (COA; 3.1%), Taiwanese Society of Endoscopy Spine Surgery (3.1%), AO Spine (3.9%), the Arab Spine Society (0.8%), and others, such as Asean MIST, the Mexican Spine Society – AMCICO (3.1%), Thai Minimally Invasive Spine Society (ThaiMISST; 1.6%), Federation of Latin American Neurosurgery Societies (FLANC 1.6%), Swiss Spine and Swiss Neurosurgical Society (0.6%), Deutsche Wirbelsaulengesellschaft (DWG; 0.6%), and Saudi Association of Neurosurgery (0.8%).

Most surgeons were members of professional surgeons organizations including the North American Spine Society (NASS; 26.8%), The Brazilian Spine Society – Sociedade Brasiliera de Columna (SBC; 22%), Inter-American Society for Minimally Invasive Spine Surgery – Sociedad Interamericana de Cirurgia de Columna Minimamente Invasiva (SICCMI; 14.2$), American Association of Neurological Surgeons (AANS; 12.6%), American Academy of Orthopedic Surgeons (AAOS; 12.6%), Society For Minimally Invasive Spine Surgery (SMISS; 12.6%), Congress of Neurological Surgeons (CNS; 11.8%), Sociedad Iberolatinoamericana de Columna (SILACO; 11.0%), Korean Minimally Invasive Spine Society (KOMISS; 8.7%), International Society For The Advancement of Spine Surgery (ISASS; 7.9%), European Spine Society (7.1%), Korean Endoscopic Spine Society (KOSESS; 5.5%), KOMISS (8.7%) American Medical Association (AMA; 3.9%), International Society for Minimal Intervention in Spinal Surgery (ISMISS; 3.9%), Chinese Orthopedic Association (COA; 3.1%), Taiwanese Society of Endoscopy Spine Surgery (TSESS; 3.1%), AO Spine (3.9%), the Arab Spine Society (0.8%), and others, such as Asean MIST, the Mexican Spine Society – Associacion Mexicana de Cirujanos de Columna (AMCICO; 3.1%), Thai Minimally Invasive Spine Society (ThaiMISST; 1.6%), Federation of Latin American Neurosurgery Societies (FLANC 1.6%), Swiss Spine and Swiss Neurosurgical Society (0.6%), Deutsche Wirbelsaulengesellschaft (DWG; 0.6%), and Saudi Association of Neurosurgery (0.8%).
The raw response data regarding the learning curve, psychological stress, risk taking, and mental effort, as well as work-related RVU assessments, are listed in Tables 2–4. The lower complexity procedures with lower reimbursement are listed at the top of each of these tables. Interestingly, more than two-thirds of responding surgeons indicated that spinal endoscopy was either just as hard or much harder to learn and master than several of the traditional translaminar decompression and even fusion procedures. The psychological stress and mental and work effort were also assessed as high at more than 50% for most of the comparator surgeries except the instrumented fusion operation.
Physician learning curve comparisons.
Physician mental effort, procedure intensity, and psychological stress comparisons.
Physician work comparison.
The IRT dichotomous Rasch analysis was employed to assess the learning curve difficulty of endoscopic lumbar decompression surgery compared with other commonly performed spinal surgeries (Table 1). The data were graphically displayed in the resulting Wright plots (Figures 6–8). On the left of the Wright plot, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability. The responding surgeons represented by horizontal bars at the top indicated that endoscopic spinal surgery is more complex to learn (positive logits) than those on the bottom (negative logits). On the right, the more challenging comparator surgeries are listed at the top vs the less challenging ones on the bottom. Directly across from 0, those surgeons had a 50% chance of considering the learning curve with endoscopic spine surgery as harder, more stressful, or associated with higher work effort than those described by the comparator CPT code.

The item response theory (IRT) dichotomous Rasch analysis was employed to assess the learning curve difficulty of endoscopic lumbar decompression surgery compared with other commonly performed spinal surgeries (Table 1). Shown is the resulting Wright plot. On the left, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability. The surgeons represented by horizontal bars at the top indicated that endoscopic spinal surgery is more complex to learn (positive logits) than those on the bottom (negative logits). On the right, the more challenging comparator surgeries are listed at the top vs the less challenging ones on the bottom. Directly across from 0, those surgeons had a 50% chance of considering the learning curve with endoscopic spine surgery as harder than those described by the comparator CPT code. One logit above suggests an approximately 75% chance that these comparator surgeries were considered more challenging than lumbar endoscopic surgery vs one logit below, which suggests an approximately 25% chance that the comparator surgeries were considered more straightforward than lumbar endoscopic surgery. There were assessment gaps above CPT code 63620 and below CPT code 63005. There were areas of redundancy with CPT codes 22102, 63005, 63047, 63030, 22532, and 22633, suggesting a similar degree of learning curve effort between these surgeries.

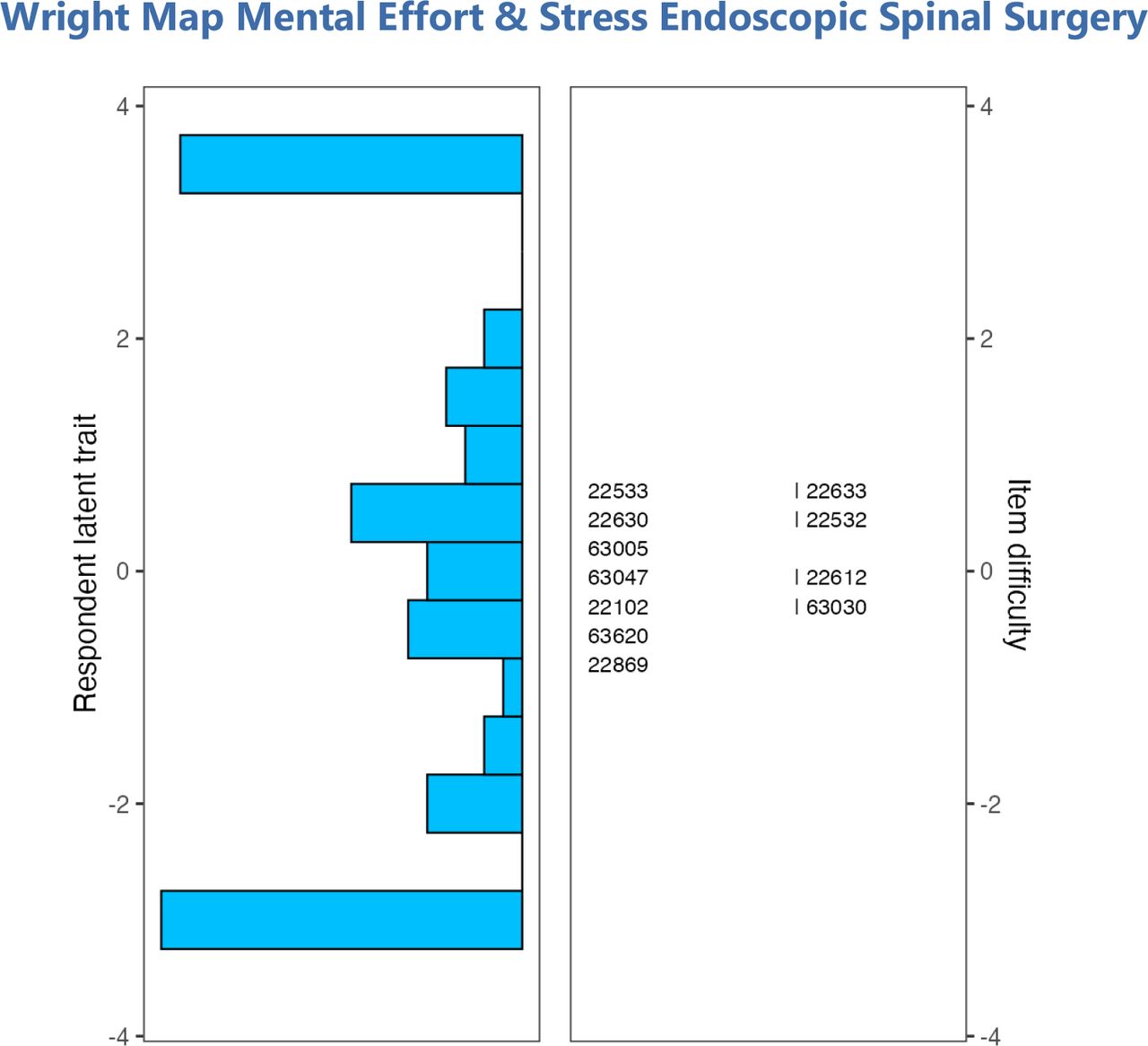
The item response theory (IRT) dichotomous Rasch analysis was employed to assess the mental effort and psychological stress of endoscopic lumbar decompression surgery compared with other commonly performed spinal surgeries (Table 1). Shown is the resulting Wright plot. On the left, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon mental effort-related stress. The surgeons represented by horizontal bars at the top indicated that endoscopic spinal surgery is more stressful (positive logits) than those on the bottom (negative logits). On the right, the more stressful comparator surgeries are listed at the top vs the less stressful ones on the bottom. Directly across from 0, those surgeons had a 50% chance of considering the mental effort and psychological stress with endoscopic spine surgery as higher than those described by the comparator CPT code. One logit above suggests an approximately 75% chance that these comparator surgeries were considered more stressful than lumbar endoscopic surgery vs one logit below suggests an approximately 25% chance that the comparator surgeries were considered less stressful than lumbar endoscopic surgery. There were assessment gaps above CPT code 22533 and below CPT code 22869. There were areas of redundancy with CPT codes 22533, 22633, 22630, 22532, 22102, and 63030, suggesting a similar degree of stress between these surgeries.

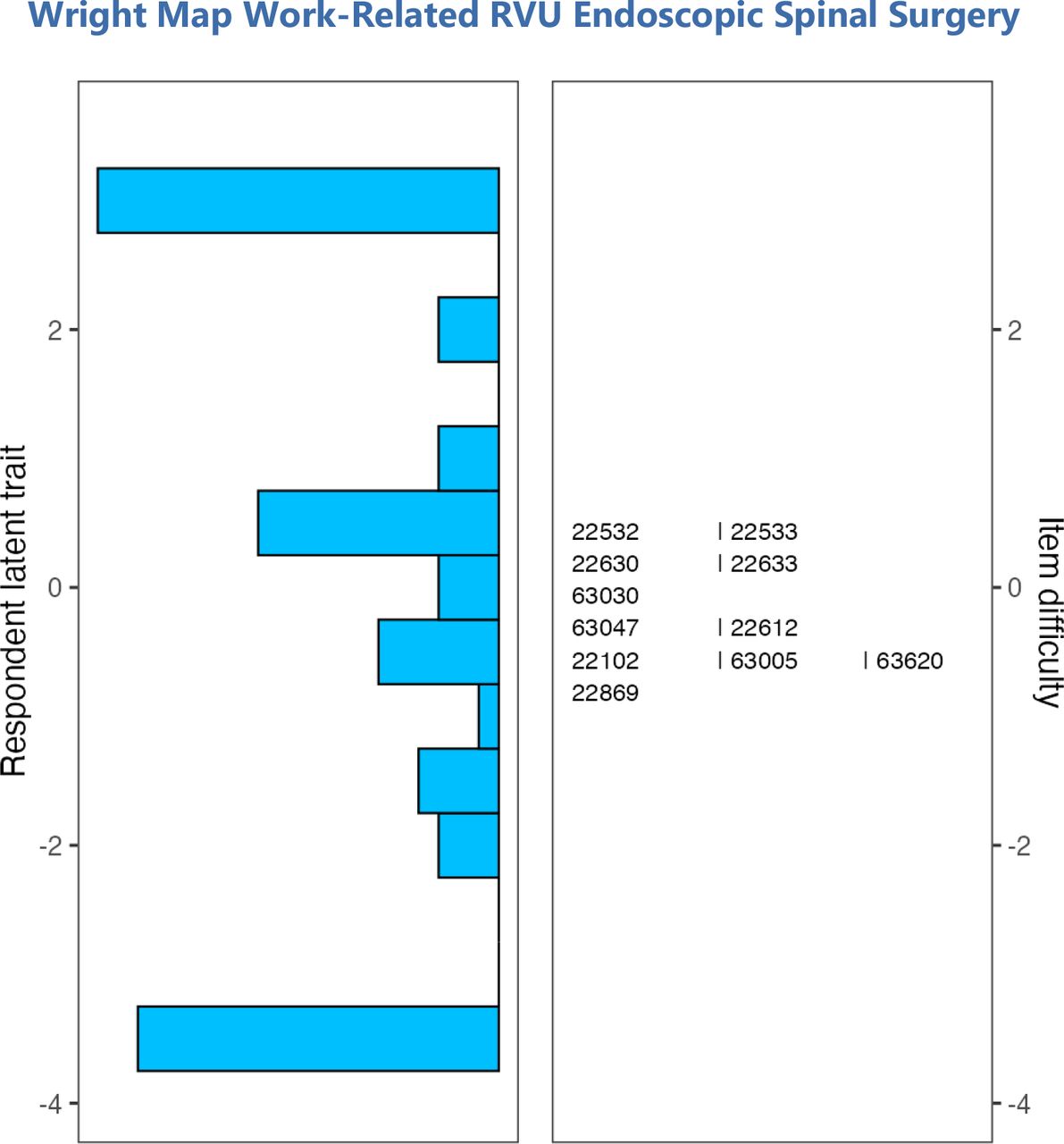
The item response theory (IRT) dichotomous Rasch analysis was employed to assess the work effort difficulty of endoscopic lumbar decompression surgery compared with other commonly performed spinal surgeries (Table 1). Shown is the resulting Wright plot. On the left, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability. The surgeons represented by horizontal bars at the top of the chart indicated that endoscopic spinal surgery requires more work effort (positive logits) than those on the bottom (negative logits). On the right, the more challenging comparator surgeries are listed at the top vs the less challenging ones on the bottom. Directly across from 0, those surgeons had a 50% chance of considering the work effort with endoscopic spine surgery as harder than those described by the comparator CPT code. One logit above suggests an approximately 75% chance that these comparator surgeries were considered more work than lumbar endoscopic surgery vs one logit below suggests an approximately 25% chance that the comparator surgeries were considered less work than lumbar endoscopic surgery. There were assessment gaps above CPT code 22532 and below CPT code 22869. There were areas of redundancy with CPT codes 22102, 63620, 22869, 63047, 22612, 22532, and 22533, suggesting a similar degree of difficulty between these surgeries.
The learning curve Wright plot (Figure 6) showed higher odds—measures with infit and outfit statistics listed in Table 5—with reasonable reliability (0.691) that the lumbar endoscopic decompression surgery is more challenging to learn than the traditional translaminar lumbar decompression procedures, such as laminectomy and microsurgical hemilaminotomy discectomy, and even some of the lumbar fusion surgeries described by CPT codes 63620, 22532, 63047, 63030, and 22633. There were assessment gaps above CPT 63620 and below CPT 63005. There were areas of redundancy with CPT 22102 and CPT 63005, CPT 63047, CPT 63030, CPT 22532, and CPT 22633, suggesting a similar degree of learning curve effort between these surgeries. The psychological stress and mental effort Wright plot (Figure 7) showed higher odds—measures with infit and outfit statistics listed in Table 6—with good reliability (0.762) that the lumbar endoscopic decompression surgery is more stressful than the fusion procedures, including the posterior lumbar interbody fusion (PLIF) described by CPT codes 22532, 22533, 22633, 22630, 63005, and 63047. There were assessment gaps above CPT 22533 and below CPT 22869. There were areas of redundancy with CPT 22533, CPT 22633, CPT 22630, CPT 22532, CPT 22102, and CPT 63030, suggesting a similar degree of stress between these surgeries. The work-related effort Wright plot (Figure 8) showed higher odds—measures with infit and outfit statistics listed in Table 7—with good reliability (0.764) that the lumbar endoscopic decompression surgery is associated with higher work effort than the fusion procedures described by CPT codes 22532 and 22533 (extracavitary thoracic and lumbar fusion), and CPT codes 22630 (PLIF) and 22633 (PLIF combined with posterolateral fusion), and the traditional translaminar decompression surgeries described by CPT codes 63047 (laminectomy) and 63030 (hemilaminectomy with discectomy). There were assessment gaps above CPT code 22532 and below CPT code 22869. There were areas of redundancy with CPT codes 22102, 63620, 22869, 63047, 22612, 22532, and 22533, suggesting a similar degree of difficulty between these surgeries.
Dichotomous Rasch model analysis learning curve endoscopic lumbar decompression.
Dichotomous Rasch model analysis of psychological stress and mental effort endoscopic lumbar decompression.
Dichotomous Rasch model analysis work effort endoscopic lumbar decompression.
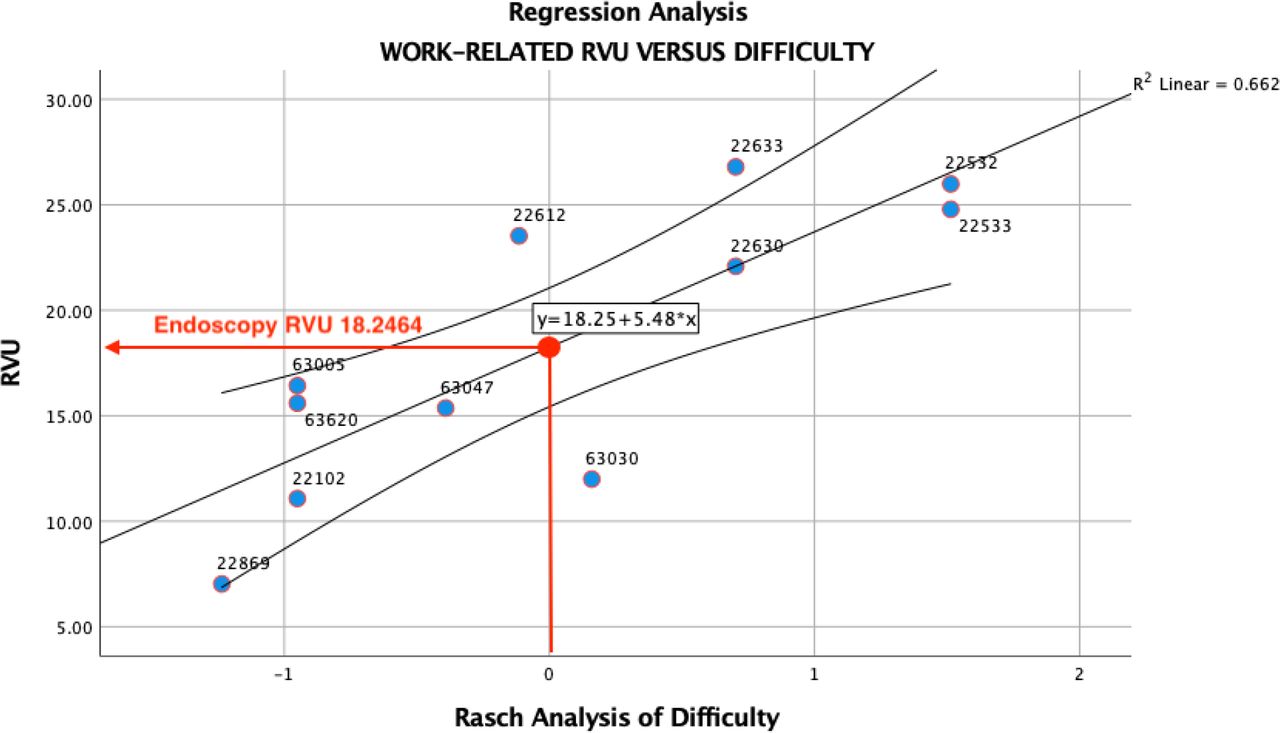
Linear regression of work-related RVUs vs Rasch analysis of difficulty of the various comparator lumbar spinal surgeries vs the lumbar endoscopic decompression is shown in Figure 9. The Rasch analysis of surgeon ability and procedural difficulty allowed the determination of the appropriately valued RVU number for the lumbar endoscopic decompression procedure at the zero logit point as 18.2464.

Linear regression scatter plot with mean 95% confidence interval of work-related RVUs vs difficulty of comparator spinal surgeries described by the comparator CPT codes. The Rasch analysis of surgeon ability and procedural difficulty allowed the determination of the appropriately valued RVU number for the lumbar endoscopic decompression procedure at the zero logit point as 18.2464.
Discussion
ISASS was accepted as a member of the AMA House of Delegates at their June 2014 meeting. Since then, ISASS has actively participated in various RUC meetings to advocate for the accurate valuation of several CPT codes crucial to spine surgeons’ reimbursement for common lumbar spinal decompression and fusion procedures. For example, the 2014 misevaluation of CPT 27279 (minimally invasive sacroiliac joint arthrodesis) was eventually revised. In order to address the work RVU assigned to CPT 27279, ISASS requested refinement of the code in December 2014 through a process convened by CMS. CMS grants requests for a refinement panel for codes with interim values where new data were not available at the time when the code went through the RUC process, as it might inform CMS before the value is finalized via the final Physician Fee Schedule rulemaking of misvaluations. In order to present new data to CMS, this team of ISASS member authors supported by a wide array of member surgeons of other societies, such as the North American Spine Society, the American Association of Orthopedic Surgeons, and the American Association of Neurological Surgeons, and member surgeons of several other well recognized international societies, such as KOMISS, KOSSES, SBN, SBC, SICCMI, AMCICO, the European Spine Society, AO Spine, and others (Table 1), utilized an alternative process to evaluate the learning curve, the psychological stress, and the mental and work effort using the Rasch methodology to assess the data of a surgeon survey.
In its original application, the Rasch approach utilizes the Poisson distribution to depict errors students commit during textual reading. Rasch termed this as the multiplicative Poisson model. Subsequently, he introduced the Rasch model tailored for dichotomous data, applying it to intelligence and performance test results, including datasets from the Danish military. Concurrently, American researchers pioneered the IRT. Within the IRT framework, the Rasch model is one of the most fundamental response configurations. Unlike other foundational models, the Rasch model possesses a unique mathematical characteristic: its parameters (such as item challenges and test-taker capabilities) are deemed adequate statistics. Rasch substantiated that his methodology aligned with measurement standards derived from physical science evaluations. The Rasch model holds significant prominence in educational and psychological assessments, especially in gauging attainment and cognitive capabilities. The authors of this study used it to ultimately recommend the appropriate valuation of the lumbar endoscopic decompression surgery described in CPT code 62380, which to this date has not received an RVU value. This research methodology received endorsements from various esteemed organizations including the Interamerican Society for Minimally Invasive Spine Surgery (SICCMI), the Mexican Society of Spinal Surgeons (AMCICO), the International Society for Minimally Invasive Spine Surgery (ISMISS), the Brazilian Spine Society (SBC), the Society for Minimally Invasive Spine Surgery (SMISS), the Korean Minimally Invasive Spine Surgery (KOMISS), and the International Society for the Advancement of Spine Surgery (ISASS).
The results of the Rasch analysis are underpinned with statistical proof what is common knowledge among spine surgeons. The learning curve with lumbar endoscopic spinal surgery is steeper and more complex than with traditional translaminar lumbar decompression surgeries, such as laminectomy and hemilaminectomy with discectomy and microsurgical dissection and in some instances even steeper than with posterior lumbar interbody and posterolateral fusion surgeries. Similarly, the Rasch analysis proved that the psychological stress and mental and work effort with the lumbar endoscopic decompression surgery are perceived higher by responding spine surgeons compared with posterior decompression surgeries and even posterior interbody and posterolateral fusion surgeries. The regression analysis of work effort vs procedural difficulty showed the real-world evaluation of the lumbar endoscopic decompression surgery described in CPT code 62380. The authors determined that RVU should be valued at 18.2464 as currently listed in the code’s description. This valuation is approximately 111.1% of the laminectomy with exploration and/or decompression of spinal cord and/or cauda equina (CPT 63005), 118.71% of the laminectomy code (CPT 63047), which includes foraminotomy and facetectomy, 152.1% of the hemilaminectomy code (CPT 63030), and 259.55% of the interlaminar or interspinous process stabilization/distraction without decompression code (CPT 22869).
Although 83.5% of responding surgeons were members of North American professional surgeon societies, it did offer an advantage by transcending national boundaries, providing insights into global surgical disparities. Although critics could argue that this Rasch analysis with global reach may have limited applicability for discussions with CMS, extending the survey globally aimed to mitigate biases and enhance understanding of the US system. Surgical care, which was historically neglected,10 is now recognized as a global health priority,11 with estimates suggesting that diseases requiring surgical care will significantly contribute to disability-adjusted life years in the near future.12 The shortage of surgeons globally highlights disparities in access to care.13,14 Unlike private payers who negotiate prices, Medicare, as a price setter, considers clinical severity and geographic differences in determining reimbursement rates.15 Therefore, considering the input from surgeons residing outside the United States with a different perspective on health care delivery was of importance to the authors.
Conclusions
The Rasch analysis suggests that the value assigned to endoscopic lumbar decompression surgery should surpass that of standard lumbar surgeries such as laminectomy and microsurgical discectomy via the hemilaminotomy approach. Future analysis might be necessary as technology advances and surgeons acquire higher skill levels, leading to the performance of more intricate endoscopic procedures, such as advanced spinal stenosis decompression or endoscopic treatment of instability with spinal fusion. Considering the elevated level of difficulty and proficiency required, these findings also bear relevance in discussion regarding the credentialing and training for spine surgeons. It is noteworthy that the surgeons with formal postgraduate training in spine surgery indicated that mastering the endoscopic procedures is more challenging, demanding higher mental and work effort, in comparison to some traditional decompression and fusion surgeries.
Footnotes
↵† on behalf of the Interamerican Society for Minimally Invasive Spine Surgery
↵‡ on behalf of the Mexican Society of Spinal Surgeons (AMCICO)
↵§ on behalf of the International Society for Minimally Invasive Spine Surgery
↵¶ on behalf of the Interamerican Society for Minimally Invasive Spine Surgery
↵†† on behalf of the Brazilian Spine Society
↵** on behalf of the Society for Minimally Invasive Spine Surgery (SMISS)
↵§§ on behalf of the Korean Minimally Invasive Spine Surgery
↵¶¶ on behalf of the International Society for the Advancement of Spine Surgery
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests There was no formal funding by private, government, or commercial funders. The participating spine centers and their authors (Center For Advanced Spine Care of Southern Arizona, Tucson, Arizona; Desert Institute of Spine Care, Phoenix, Arizona; Department of Orthopedics, Fundación Universitaria Sanitas, Bogotá, D.C., Colombia; Department of Neurosurgery, Orthopedics and Thoracic Surgery at Hospital Universitário Gaffre e Guinle, Universidade Federal do Estado do Rio de Janeiro, Rio de Janeiro, Brazil; Department of Orthopedic Surgery USP, Riberao Preto Brazil, Universitätsklinikum des Saarlandes, Klinik für Orthopädie and Neurochirurgie, Department of Orthopedic Surgery, Arabellaklinik, Munich, Germany, the Atualli Spine Care Clinica, Sao Paulo, Brazil; Cape Cod Health care, Hyannis, MA, USA; Department of Neurosurgery, Azienda Ospedaliero Universitaria Pisana, University of Pisa, Italy; Clínica Articulare, Belem, Brazil; Comprehensive Specialty Care, Clinical Radiology of Oklahoma, Department of Orthopedics, First Medical Center, PLA General Hospital, Beijing; Spinartus Hospital Chungdam, Korea; Department of Neurosurgery, Seoul; St. Mary’s Hospital, College of Medicine, The Catholic University of Korea) volunteered their time and internal resources to support the design and conduction of this research study. All authors aided in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. The authors declare no conflict of interest relevant to this research, and there was no personal circumstance or interest that may be perceived as inappropriately influencing the representation or interpretation of reported research results. This research was not compiled to enrich anyone. It was merely intended to advance the understanding of the learning curve, difficulty, psychological intensity, and estimated work relative value units of endoscopic lumbar spinal decompression surgery in comparison to other common lumbar spine surgeries.
Disclaimer The statements, opinions, and data contained in all publications are solely those of the individual authors and not of the editors.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2024 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}