


Article Figures & Data
Figures
- Figure 1
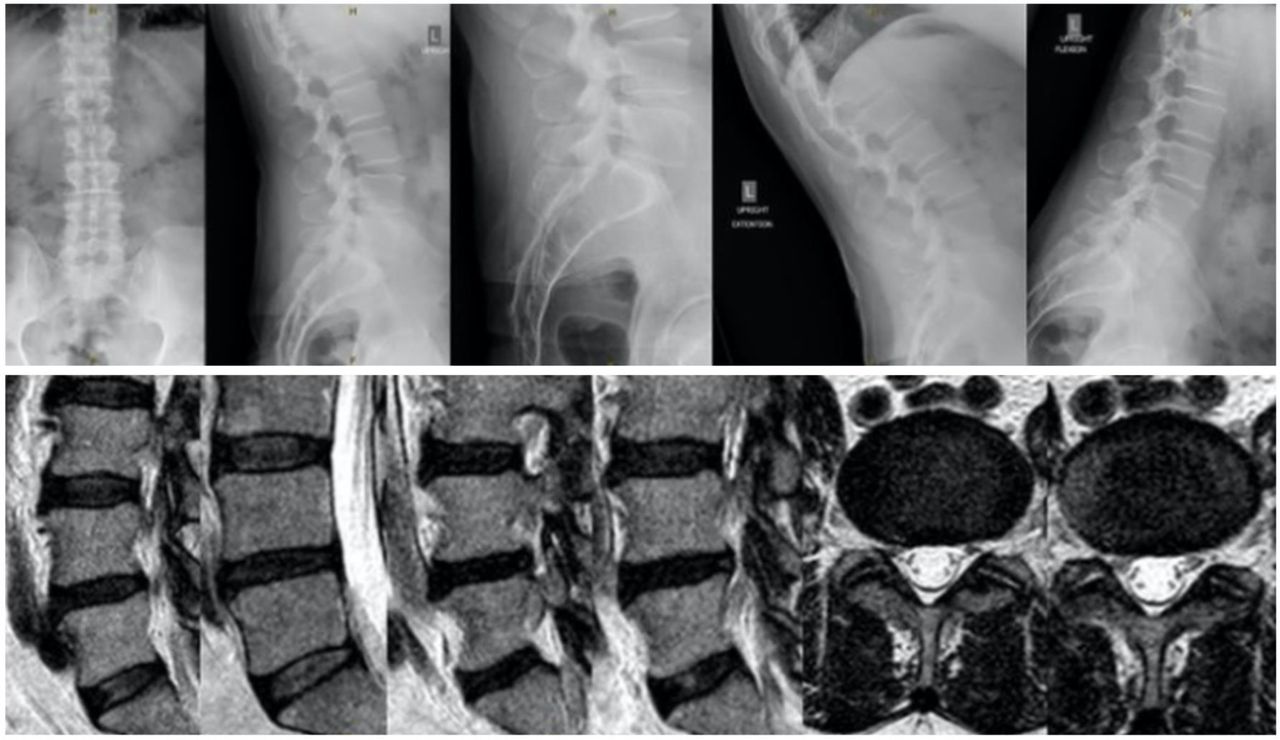
A 67-year-old man with an L4/L5 spinal stenosis causing right leg pain due to neurogenic claudication without back pain. Conservative treatments have been exhausted and failed. Imaging demonstrates foraminal and lateral spinal stenosis. An endoscopic decompression of L4/L5 foramen and the lateral canal is contemplated with the endoscopic technique of your choice.
- Figure 2
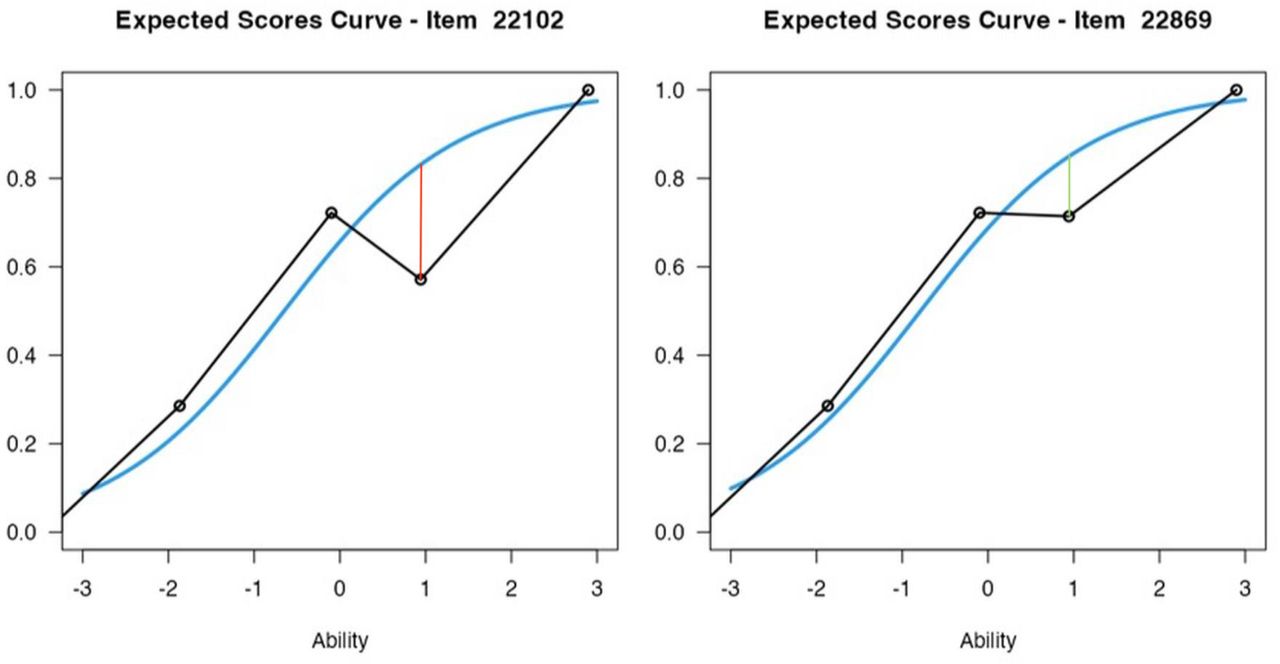
Two examples of outlier-sensitive means statistics (outfit analysis) based on the conventional sum of squared standardized residuals, which is more sensitive to unexpected observations, are shown. Surgeon responses on the difficulty of Current Procedural Terminology (CPT) code 22102 compared with the lumbar endoscopy procedure showed a greater outfit from the model predicted by the Rasch analysis (indicated by the red vertical line) than for CPT code 22869 (green vertical line), thereby suggesting the presence of confounding factors affecting responses on item for CPT code 22102. Infit (not shown in this graph) and outfit data between 0.6 and 1.4 indicate a good fit of the Rasch model. Outside these parameters, confounding factors are likely.
- Figure 3
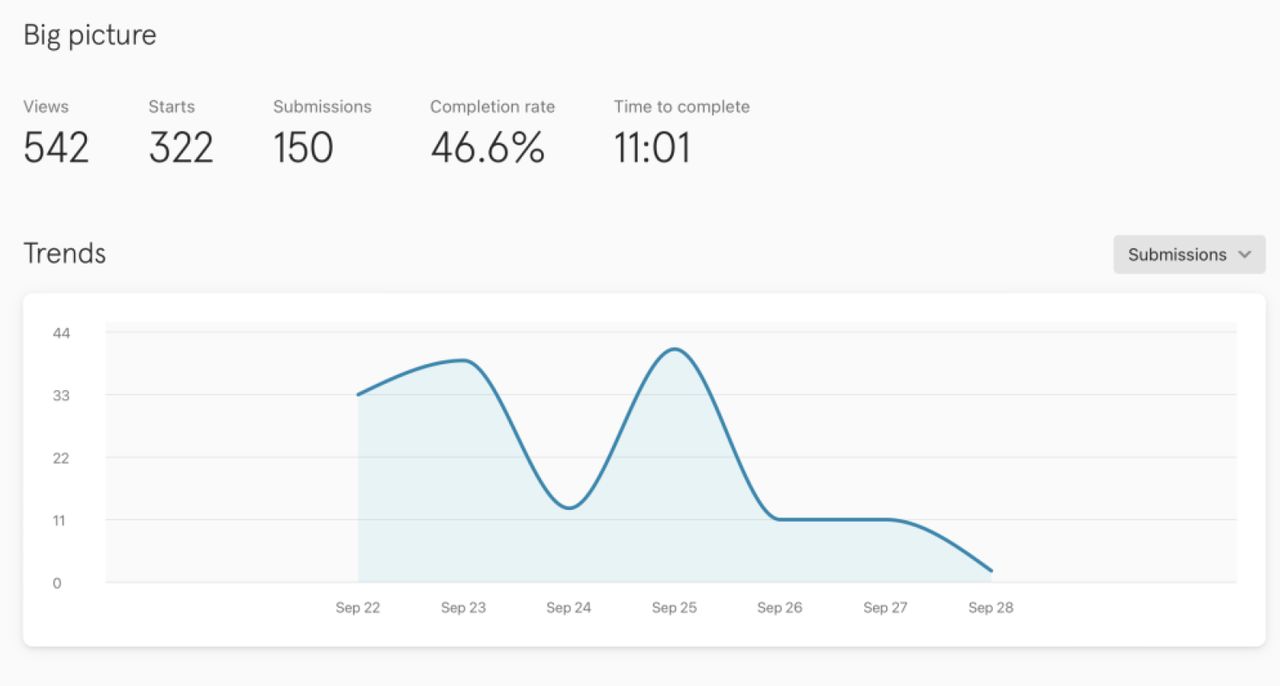
Five hundred forty-two spine surgeons accessed the online survey aimed to obtain objective measures of the learning curve effort to obtain adequate skill level to perform the endoscopic lumbar decompression operation, its psychological intensity and stress on the surgeon, and its associated work effort in comparison to other commonly performed lumbar spinal surgeries based on the input of spine surgeons who perform these procedures. Three hundred twenty-two surgeons started the survey, and 150 submitted a valid survey recording, yielding a completion rate of 43.1%.
- Figure 4
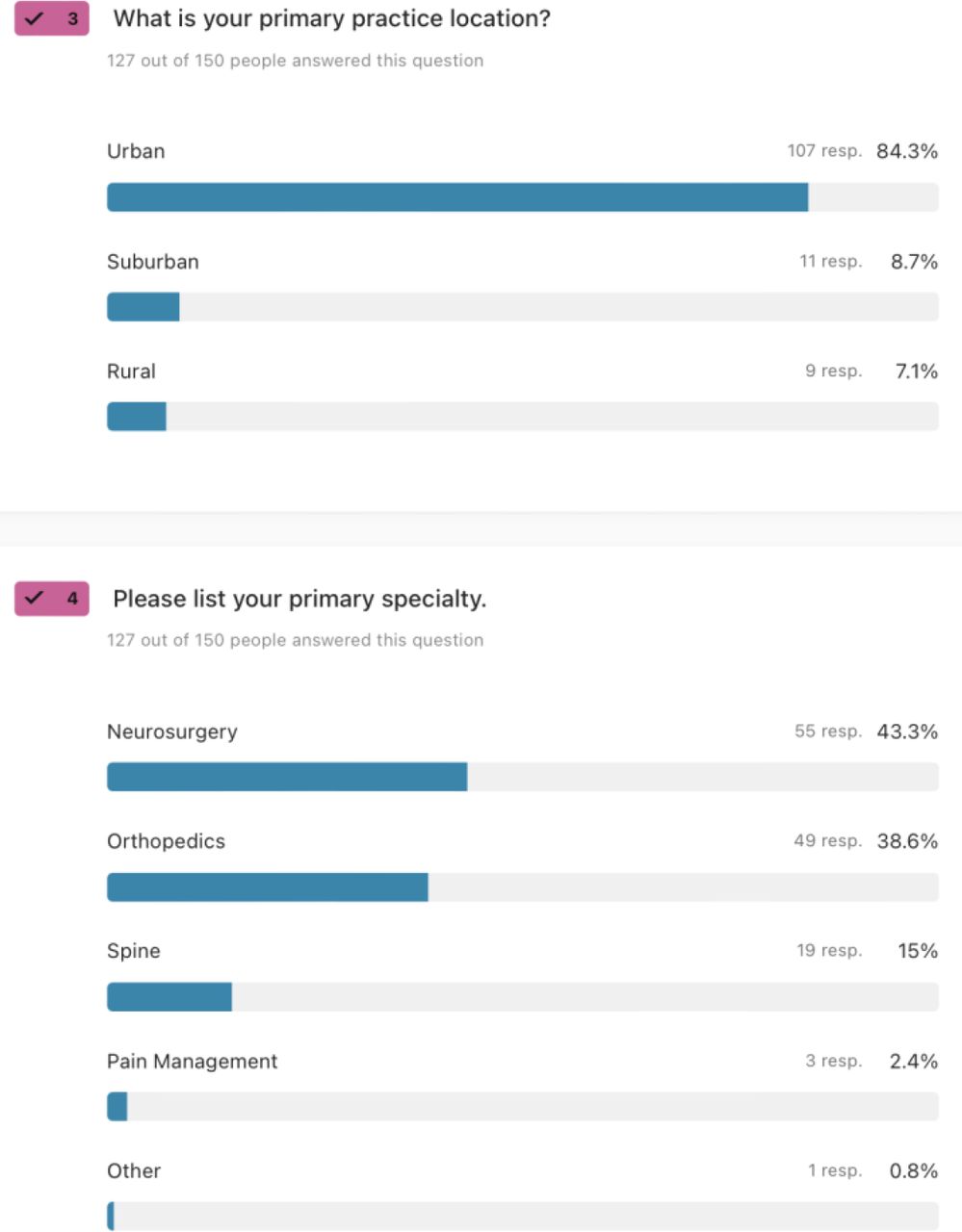
The majority of responding spine surgeons were neurosurgeons (43.3%). Orthopedic surgeons comprised 38.6% of the respondents, followed by 15% of surgeons who dedicated their practice entirely to the spine. Only 2.4% of the response came from pain management physicians. Therefore, 96.9% of respondents had a postgraduate education in a surgical specialty. Of the 150 responding surgeons, 84.3% worked in an urban practice setting, 8.7% worked in a suburban environment, followed by 7.1% who worked in a rural area.
- Figure 5
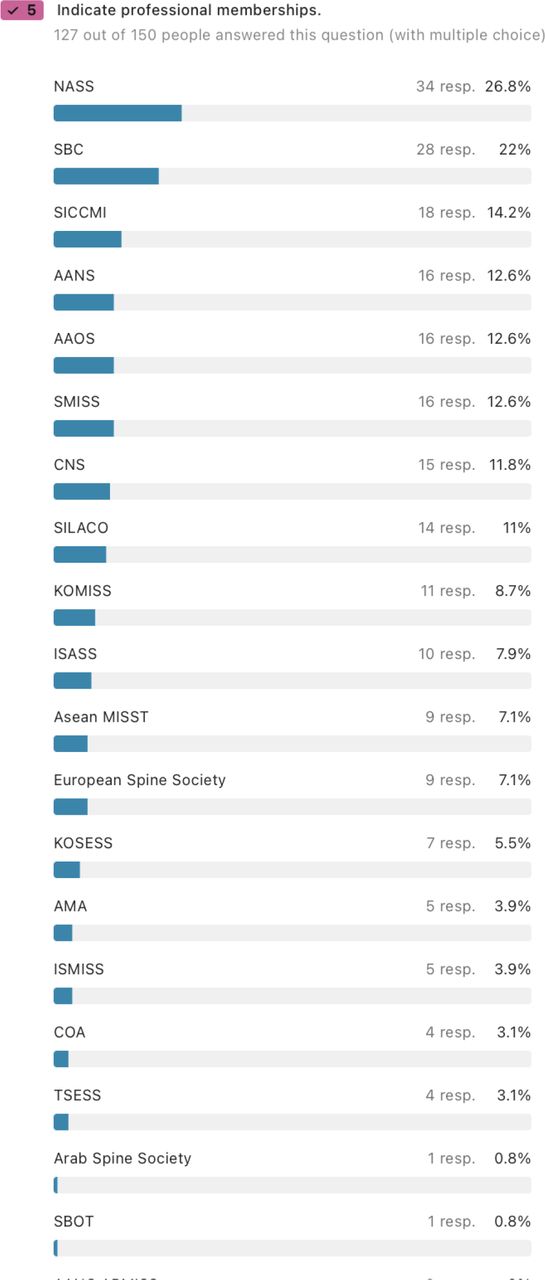
Most surgeons were members of professional surgeons organizations including the North American Spine Society (NASS; 26.8%), The Brazilian Spine Society – Sociedade Brasiliera de Columna (SBC; 22%), Inter-American Society for Minimally Invasive Spine Surgery – Sociedad Interamericana de Cirurgia de Columna Minimamente Invasiva (SICCMI; 14.2$), American Association of Neurological Surgeons (AANS; 12.6%), American Academy of Orthopedic Surgeons (AAOS; 12.6%), Society For Minimally Invasive Spine Surgery (SMISS; 12.6%), Congress of Neurological Surgeons (CNS; 11.8%), Sociedad Iberolatinoamericana de Columna (SILACO; 11.0%), Korean Minimally Invasive Spine Society (KOMISS; 8.7%), International Society For The Advancement of Spine Surgery (ISASS; 7.9%), European Spine Society (7.1%), Korean Endoscopic Spine Society (KOSESS; 5.5%), KOMISS (8.7%) American Medical Association (AMA; 3.9%), International Society for Minimal Intervention in Spinal Surgery (ISMISS; 3.9%), Chinese Orthopedic Association (COA; 3.1%), Taiwanese Society of Endoscopy Spine Surgery (TSESS; 3.1%), AO Spine (3.9%), the Arab Spine Society (0.8%), and others, such as Asean MIST, the Mexican Spine Society – Associacion Mexicana de Cirujanos de Columna (AMCICO; 3.1%), Thai Minimally Invasive Spine Society (ThaiMISST; 1.6%), Federation of Latin American Neurosurgery Societies (FLANC 1.6%), Swiss Spine and Swiss Neurosurgical Society (0.6%), Deutsche Wirbelsaulengesellschaft (DWG; 0.6%), and Saudi Association of Neurosurgery (0.8%).
- Figure 6
The item response theory (IRT) dichotomous Rasch analysis was employed to assess the learning curve difficulty of endoscopic lumbar decompression surgery compared with other commonly performed spinal surgeries (Table 1). Shown is the resulting Wright plot. On the left, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability. The surgeons represented by horizontal bars at the top indicated that endoscopic spinal surgery is more complex to learn (positive logits) than those on the bottom (negative logits). On the right, the more challenging comparator surgeries are listed at the top vs the less challenging ones on the bottom. Directly across from 0, those surgeons had a 50% chance of considering the learning curve with endoscopic spine surgery as harder than those described by the comparator CPT code. One logit above suggests an approximately 75% chance that these comparator surgeries were considered more challenging than lumbar endoscopic surgery vs one logit below, which suggests an approximately 25% chance that the comparator surgeries were considered more straightforward than lumbar endoscopic surgery. There were assessment gaps above CPT code 63620 and below CPT code 63005. There were areas of redundancy with CPT codes 22102, 63005, 63047, 63030, 22532, and 22633, suggesting a similar degree of learning curve effort between these surgeries.
- Figure 7
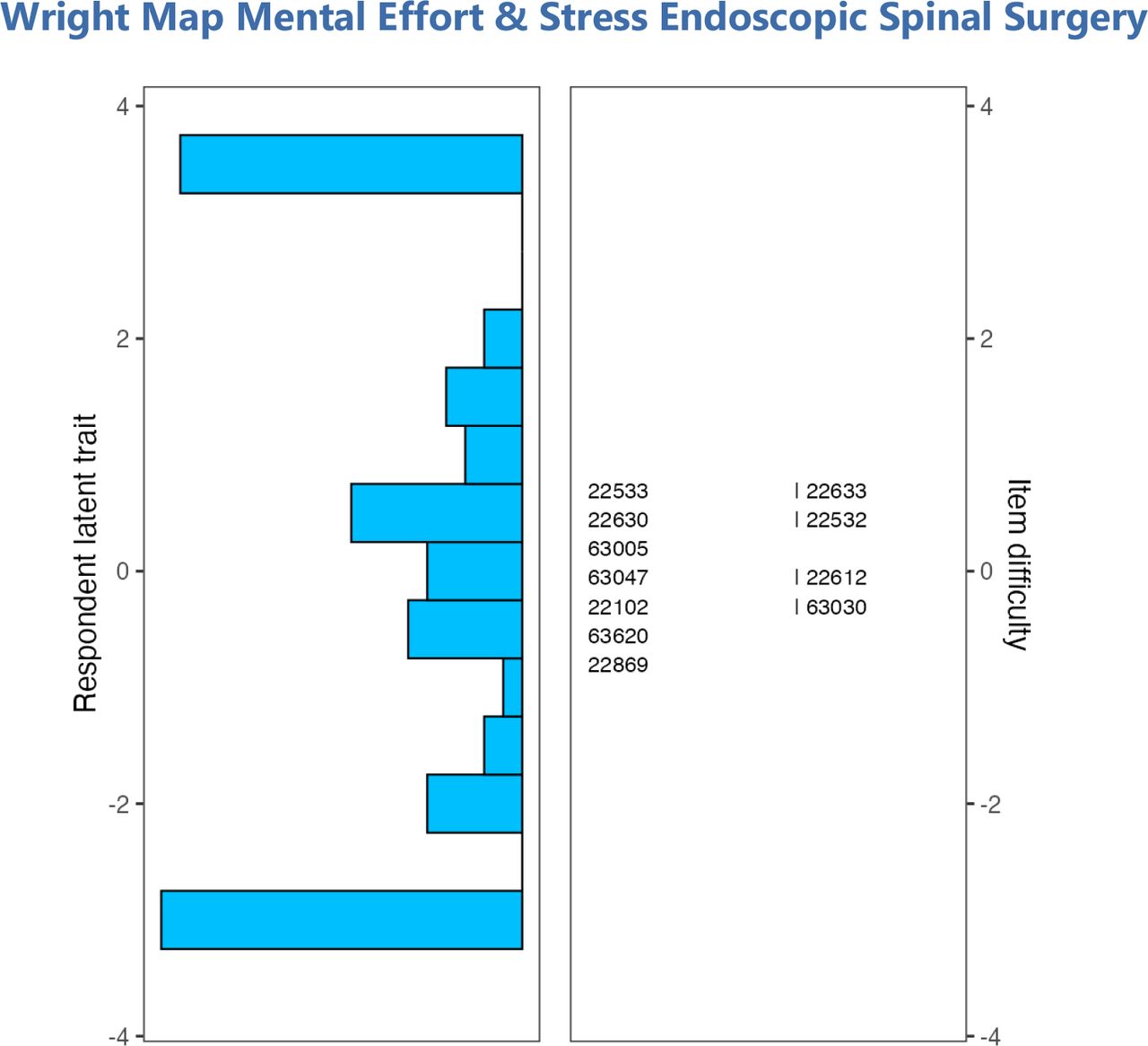
The item response theory (IRT) dichotomous Rasch analysis was employed to assess the mental effort and psychological stress of endoscopic lumbar decompression surgery compared with other commonly performed spinal surgeries (Table 1). Shown is the resulting Wright plot. On the left, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon mental effort-related stress. The surgeons represented by horizontal bars at the top indicated that endoscopic spinal surgery is more stressful (positive logits) than those on the bottom (negative logits). On the right, the more stressful comparator surgeries are listed at the top vs the less stressful ones on the bottom. Directly across from 0, those surgeons had a 50% chance of considering the mental effort and psychological stress with endoscopic spine surgery as higher than those described by the comparator CPT code. One logit above suggests an approximately 75% chance that these comparator surgeries were considered more stressful than lumbar endoscopic surgery vs one logit below suggests an approximately 25% chance that the comparator surgeries were considered less stressful than lumbar endoscopic surgery. There were assessment gaps above CPT code 22533 and below CPT code 22869. There were areas of redundancy with CPT codes 22533, 22633, 22630, 22532, 22102, and 63030, suggesting a similar degree of stress between these surgeries.
- Figure 8
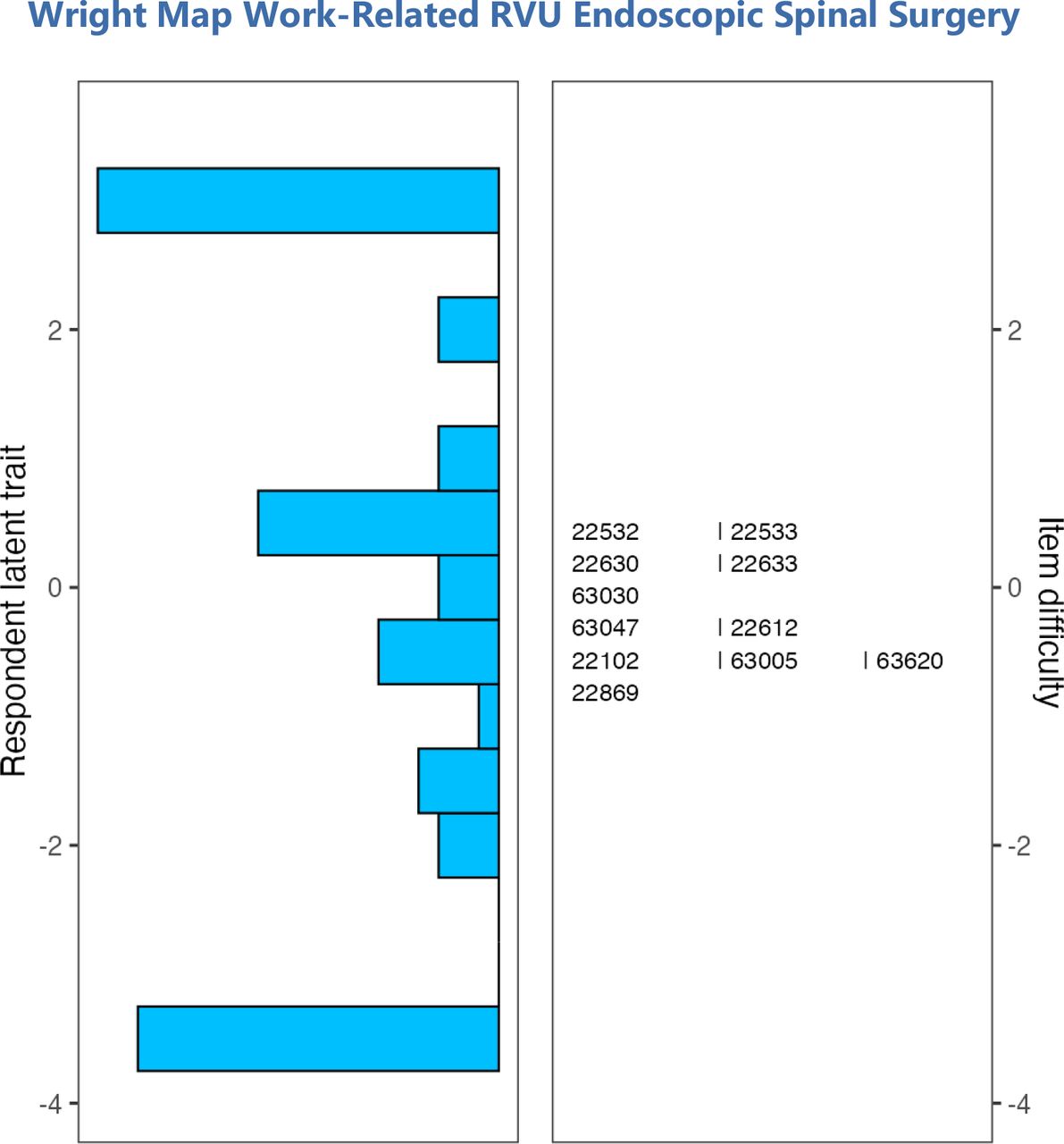
The item response theory (IRT) dichotomous Rasch analysis was employed to assess the work effort difficulty of endoscopic lumbar decompression surgery compared with other commonly performed spinal surgeries (Table 1). Shown is the resulting Wright plot. On the left, the responding surgeons’ latent traits are written in logits (log odds) as estimates of true intervals of item difficulty and surgeon ability. The surgeons represented by horizontal bars at the top of the chart indicated that endoscopic spinal surgery requires more work effort (positive logits) than those on the bottom (negative logits). On the right, the more challenging comparator surgeries are listed at the top vs the less challenging ones on the bottom. Directly across from 0, those surgeons had a 50% chance of considering the work effort with endoscopic spine surgery as harder than those described by the comparator CPT code. One logit above suggests an approximately 75% chance that these comparator surgeries were considered more work than lumbar endoscopic surgery vs one logit below suggests an approximately 25% chance that the comparator surgeries were considered less work than lumbar endoscopic surgery. There were assessment gaps above CPT code 22532 and below CPT code 22869. There were areas of redundancy with CPT codes 22102, 63620, 22869, 63047, 22612, 22532, and 22533, suggesting a similar degree of difficulty between these surgeries.
- Figure 9
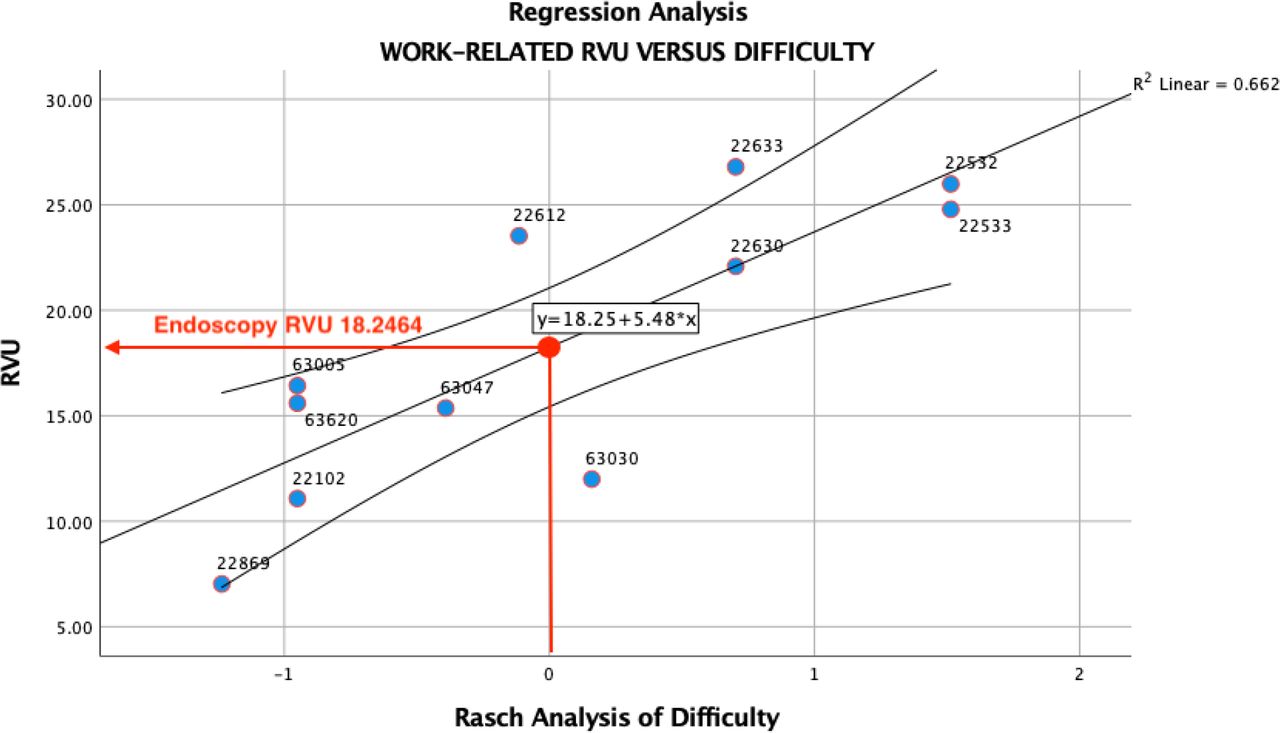
Linear regression scatter plot with mean 95% confidence interval of work-related RVUs vs difficulty of comparator spinal surgeries described by the comparator CPT codes. The Rasch analysis of surgeon ability and procedural difficulty allowed the determination of the appropriately valued RVU number for the lumbar endoscopic decompression procedure at the zero logit point as 18.2464.









Tables
CPT Code Descriptor Work RVUs 22869 Insertion of interlaminar/interspinous process stabilization/distraction device, without open decompression or fusion, including image guidance when performed, lumbar; single level 7.03 22102 Partial excision of posterior vertebral component (eg, spinous process, lamina, or facet) for intrinsic bony lesion, single vertebral segment; lumbar 11.08 63030a Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar 12.00 63047 Laminectomy, facetectomy, and foraminotomy (unilateral or bilateral with decompression of spinal cord, cauda equina and/or nerve root[s], eg, spinal or lateral recess stenosis), single vertebral segment; lumbar 15.37 63620 Stereotactic radiosurgery (particle beam, gamma ray, or linear accelerator); 1 spinal lesion 15.60 63005 Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis 16.43 22630 Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar 22.09 22612 Arthrodesis, posterior, or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) 23.53 22532 Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic 25.99 22533 Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); lumbar 24.79 22633a Arthrodesis, combined posterior, or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar 26.80 Abbreviations: CPT, Current Procedural Terminology; OWCP, Office of Workers' Compensation Program; RVU, relative value unit.
Note: OWCP Medical Fee Schedule—Effective Date: 9 July 2023, Last Update: 18 September 2023.8
↵a From 2018 to the latest OWCP Medical Fee Schedule update on 18 September 2023, the RVU numbers have remained unchanged for most CPT codes listed in Table 1 except for CPT Code 63030, which was reduced from 13.18 (2018) to 12.00 (2023) and CPT code 22633, which was reduced from 27.75 (2018) to 26.80 (2023).
CPT Description (Code) Endoscopy Is EASIER to Learn Endoscopy Is HARDER to Learn Endoscopy Has an EQUAL Learning Curve I Do Not Perform This Comparative Procedure Laminectomy and Spinal Cord Decompression, Lumbar (63047) 26%
(33 responses)61.4%
(78 responses)10.2%
(13 responses)2.4%
(3 responses)Partial excision of posterior vertebral component (eg, spinous process, lamina, or facet) for intrinsic bony lesion, single vertebral segment; lumbar (22102) 22%
(28 responses)66.1%
(84 responses)7.9%
(10 responses)3.9%
(5 responses)Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace and lumbar (63030) 29.9%
(38 responses)55.9%
(71 responses)11.8%
(15 responses)2.4%
(3 responses)Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (63005) 23.6%
(30 responses)63.8%
(81 responses)8.7%
(11 responses)3.9%
(5 responses)Stereotactic radiosurgery (particle beam, gamma ray, or linear accelerator); 1 spinal lesion (63620) 22.8%
(29 responses)31.5%
(40 responses)3.9%
(5 responses)41.7%
(53 responses)Insertion of interlaminar/interspinous process stabilization/distraction device, without open decompression or fusion, including image guidance when performed, lumbar; single level (22869) 18.1%
(23 responses)46.5%
(59 responses)4.7%
(6 responses)30.7%
(39 responses)Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar (22630) 23.6%
(30 responses)61.4%
(78 responses)8.7%
(11 responses)6.3%
(8 responses)Arthrodesis, posterior or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (22612) 20.5%
(26 responses)55.9%
(71 responses)13.4%
(17 responses)10.2%
(13 responses)Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic (22532) 28.3%
(36 responses)44.9%
(57 responses)10.2%
(13 responses)16.5%
(21 responses)Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); lumbar (22533) 25.2%
(32 responses)47.2%
(60 responses)11%
(14 responses)16.5%
(21 responses)Arthrodesis, combined posterior, or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar (22633) 27.6%
(35 responses)50.4%
(64 responses)7.9%
(10 responses)14.2%
(18 responses)Abbreviation: CPT, Current Procedural Terminology.
- Table 3
Physician mental effort, procedure intensity, and psychological stress comparisons.
CPT Description (Code) Endoscopy Is EASIER to Learn Endoscopy Is HARDER to Learn Endoscopy Has an EQUAL Learning Curve I Do Not Perform This Comparative Procedure Laminectomy and Spinal Cord Decompression, Lumbar (63047) 48.8%
(62 responses)40.9%
(52 responses)7.9%
(10 responses)2.4%
(3 responses)Partial excision of posterior vertebral component (eg, spinous process, lamina, or facet) for intrinsic bony lesion, single vertebral segment; lumbar (22102) 44.9%
(57 responses)43.3%
(55 responses)8.7%
(11 responses)3.1%
(4 responses)Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy and/or excision of herniated intervertebral disc; 1 interspace, lumbar (63030) 51.2%
(65 responses)42.5%
(54 responses)4.7%
(6 responses)1.6%
(2 responses)Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (63005) 50.4%
(64 responses)41.7%
(53 responses)6.3%
(8 responses)1.6%
(2 responses)Stereotactic radiosurgery (particle beam, gamma ray, or linear accelerator); 1 spinal lesion (63620) 25.2%
(32 responses)29.9%
(38 responses)4.7%
(6 responses)40.2%
(51 responses)Insertion of interlaminar/interspinous process stabilization/distraction device, without open decompression or fusion, including image guidance when performed, lumbar; single level (22869) 26.8%
(34 responses)33.9%
(43 responses)8.7%
(11 responses)30.7%
(39 responses)Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar (22630) 43.3%
(55 responses)37.8%
(48 responses)11%
(14 responses)7.9%
(10 responses)Arthrodesis, posterior or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (22612) 37.8%
(48 responses)41.7%
(53 responses)11.8%
(15 responses)8.7%
(11 responses)Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic (22532) 39.4%
(50 responses)35.4%
(45 responses)7.9%
(10 responses)17.3%
(22 responses)Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); lumbar (22533) 42.5%
(54 responses)33.9%
(43 responses)7.1%
(9 responses)16.5%
(21 responses)Arthrodesis, combined posterior, or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar (22633) 44.1%
(56 responses)35.4%
(45 responses)10.2%
(13 responses)10.2%
13 (responses)Abbreviation: CPT, Current Procedural Terminology.
CPT Description (Code) Endoscopy Is EASIER to Learn Endoscopy Is HARDER to Learn Endoscopy Has an EQUAL Learning Curve I Do Not Perform This Comparative Procedure Laminectomy and Spinal Cord Decompression, Lumbar (63047) 43.3%
(55 responses)47.2%
(60 responses)7.9%
(10 responses)1.6%
(2 responses)Partial excision of posterior vertebral component (eg, spinous process, lamina, or facet) for intrinsic bony lesion, single vertebral segment; lumbar (22102) 40.2%
(51 responses)47.2%
(60 responses)9.4%
(12 responses)3.1%
(4 responses)Laminotomy (hemilaminectomy), with decompression of nerve root(s), including partial facetectomy, foraminotomy, and/or excision of herniated intervertebral disc; 1 interspace, lumbar (63030) 44.9%
(57 responses)42.5%
(54 responses)10.2%
(13 responses)2.4%
(3 responses)Laminectomy with exploration and/or decompression of spinal cord and/or cauda equina, without facetectomy, foraminotomy, or discectomy (eg, spinal stenosis), 1 or 2 vertebral segments; lumbar, except for spondylolisthesis (63005) 40.9%
(52 responses)48%
(61 responses)7.9%
(10 responses)3.1%
(4 responses)Stereotactic radiosurgery (particle beam, gamma ray, or linear accelerator); 1 spinal lesion (63620) 25.2%
(32 responses)27.6%
(35 responses)4.7%
(6 responses)42.5%
(54 responses)Insertion of interlaminar/interspinous process stabilization/distraction device, without open decompression or fusion, including image guidance when performed, lumbar; single level (22869) 27.6%
(35 responses)35.4%
(45 responses)7.1%
(9 responses)29.9%
(38 responses)Arthrodesis, posterior interbody technique, including laminectomy and/or discectomy to prepare interspace (other than for decompression), single interspace; lumbar (22630) 40.9%
(52 responses)44.1%
(56 responses)9.4%
(12 responses)5.5%
(7 responses)Arthrodesis, posterior, or posterolateral technique, single level; lumbar (with lateral transverse technique, when performed) (22612) 37.8%
(48 responses)44.9%
(57 responses)9.4%
(12 responses)7.9%
(10 responses)Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); thoracic (22532) 40.2%
(51 responses)35.4%
(45 responses)9.4%
(12 responses)15%
(19 responses)Arthrodesis, lateral extracavitary technique, including minimal discectomy to prepare interspace (other than for decompression); lumbar (22533) 41.7%
(53 responses)35.4%
(45 responses)8.7%
(11 responses)14.2%
(18 responses)Arthrodesis, combined posterior, or posterolateral technique with posterior interbody technique including laminectomy and/or discectomy sufficient to prepare interspace (other than for decompression), single interspace and segment; lumbar (22633) 38.6%
(49 responses)41.7%
(53 responses)10.2%
(13 responses)9.4%
(12 responses)Abbreviation: CPT, Current Procedural Terminology.
Model Fit Person Reliability MADaP3a P Scale 0.691 0.285 <0.001 Endoscopic Lumbar Learning Curve Item Statistics CPT Code Measure Infitb Outfitc 63047 −0.994 1.226 1.310 22102 −1.662 0.991 0.754 63030 −0.890 1.234 1.106 63005 −1.784 1.130 1.017 63620 −0.482 1.166 1.240 22869 −1.544 1.009 0.951 22630 −1.100 0.751 0.498 22612 −1.318 0.726 0.468 22532 −0.583 0.908 0.658 22533 −0.994 0.897 0.658 22633 −0.994 0.988 0.756 Abbreviation: CPT, Current Procedural Terminology.
↵a MADaQ3 = Mean of absolute values of centered Q_3 statistic with P value obtained by Holm adjustment
↵b Infit = Information-weighted mean square based on the χ 2 statistic with each observation weighted by its statistical information (model variance). This is more sensitive to unexpected patterns of observations by persons on items that are roughly targeted on them (and vice versa).
↵c Outfit = Outlier-sensitive means square statistic is more sensitive to unexpected observations by surgeons. Infit and outfit data between 0.6 and 1.4 indicate good fit of the Rasch model. Infit and outfit numbers outside this range suggest the presence of confounding factors, such as for CPT codes 22630 and 22612.
- Table 6
Dichotomous Rasch model analysis of psychological stress and mental effort endoscopic lumbar decompression.
Model Fit Person Reliability MADaQ3a P Scale 0.762 0.274 0.01 Lumbar Endoscopic Psychological Stress and Mental Effort Item Statistics CPT Code Measure Infitb Outfitc 63047 −0.0827 1.003 1.014 22102 −0.2090 0.867 0.617 63030 −0.2090 0.888 0.728 63005 0.2927 0.827 0.594 63620 −0.4644 1.160 0.916 22869 −0.7246 0.973 0.704 22630 0.4172 0.866 0.937 22612 −0.0827 0.689 0.375 22532 0.4172 1.104 0.792 22533 0.6667 0.919 0.542 22633 0.6667 0.956 0.607 Abbreviation: CPT, Current Procedural Terminology.
↵a MADaQ3 = Mean of absolute values of centered Q_3 statistic with P value obtained by Holm adjustment.
↵b Infit = Information-weighted mean square based on the χ 2 statistic with each observation weighted by its statistical information (model variance). This is more sensitive to unexpected patterns of observations by persons on items that are roughly targeted on them (and vice versa).
↵c Outfit = Outlier-sensitive means square statistic is more sensitive to unexpected observations by surgeons. Infit and outfit data between 0.6 and 1.4 indicate good fit of the Rasch model. Infit and outfit numbers outside this range suggest the presence of confounding factors, such as for CPT codes 63005, 22612, and 22533.
Model Fit Person Reliability MADaQ3a P Scale 0.764 0.324 <0.001 Endoscopic Lumbar RVU Work Effort Item Statistics CPT Code Measure Infitb Outfitc 63047 −0.383 0.985 0.649 22102 −0.652 1.203 0.874 63030 −0.118 0.920 0.680 63005 −0.652 0.941 0.652 63620 −0.652 1.277 1.889 22869 −0.789 0.848 0.650 22630 0.143 0.782 0.444 22612 −0.250 0.590 0.302 22532 0.533 0.906 0.953 22533 0.533 0.831 0.458 22633 0.143 0.770 0.412 Abbreviations: CPT, Current Procedural Terminology; RVU, relative value unit.
↵a MADaQ3 = Mean of absolute values of centered Q_3 statistic with P value obtained by Holm adjustment.
↵b Infit = Information-weighted mean square based on the χ 2 statistic with each observation weighted by its statistical information (model variance). This is more sensitive to unexpected patterns of observations by persons on items that are roughly targeted on them (and vice versa).
↵c Outfit = Outlier-sensitive means square statistic is more sensitive to unexpected observations by surgeons. Infit and outfit data between 0.6 and 1.4 indicate good fit of the Rasch model. Infit and outfit numbers outside this range suggest the presence of confounding factors, such as for CPT codes 22630, 22633, and 22612.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}