


Abstract
Background Only a small number of studies have offered normative data for the upper cervical spine in children and with some variation in findings.
Objective The aim of this study was to determine normal values for upper cervical spine measurements used in the assessment of upper cervical spine trauma in the pediatric population.
Methods One-hundred computed tomographic images of the cervical spine of children aged ≤16 years were included for analysis. All children were cleared of spinal injury. Anterior atlanto-dens interval (ADI), posterior atlanto-dens interval (PADI), basion-dens interval (BDI), Powers ratio, condylar-C1 interval (CCI), and lateral mass interval (LMI) were measured on the relevant sagittal or coronal images. Measurements for CCI and LMI were taken on each side.
Results Mean age was 111 months (range 11–196 months). Sixty-two were male. Mean values (and ranges) of the measurements were as follows: BDI: 7.1 mm (3.6–12.2); ADI 2.8 mm (0.8–4.8); PADI 18.7 mm (14.1–23.2); Powers ratio 0.72 (0.59–1.0); CCI 2.0 and 2.0 (0.5–4.2); and LMI 3.2 and 3.3 mm (1.7–4.8). BDI (r = −0.488), ADI (r = −0.201), PADI (r = 0.264), and CCI (r = −0.468 and −0.454) all showed significant correlation with age. The Powers ratio was the most stable measurement across all age groups.
Conclusions Normal values were reported from a local pediatric population with a wide age range. Most values correlate with age to a degree, and so normal values may vary throughout childhood. A multicenter study is desirable to advance knowledge in this field.
Clinical Relevance Current radiographic measures used to assess for possible ligamentous injury in the pediatric upper cervical spine correlate with age. Caution must be held when analyzing the upper cervical spine across a range of age groups in children.
Level of Evidence 4.
Introduction
Spinal trauma in the pediatric population is relatively rare and injury patterns are markedly different from those seen in adults.1 The pediatric spine is mobile and less susceptible to fracture than the adult spine; instead, ligamentous injuries predominate and a high index of suspicion is needed when assessing a child with possible spinal injury.2–7 Injuries to the upper cervical spine (C0–C2) present a significant challenge for the clinician; variations in anatomy here are not infrequent and the skeleton may be at varying stages of ossification resulting in imaging that is difficult to interpret.3,6 A low threshold is needed for additional advanced imaging to detect injury as missed or delayed diagnoses may have serious or even catastrophic consequences.5,8
Following modern principles of major trauma assessment, radiologic assessment of spinal trauma often includes the use of computed tomography (CT). Although conferring an increased radiation dose compared to plain radiography, CT provides more detail in multiple planes and with appropriate windows can also give detail about soft tissue injury albeit not to the same sensitivity as magnetic resonance imaging (MRI). When assessing potential injury in the upper cervical spine, advanced imaging that allows assessment of the various articulation in multiple planes at once is essential.
Established measures are available to assess the integrity of the major ligamentous stabilizers of the upper cervical spine, and normative data are available for the adult population. However, a major limitation of radiologic investigation is the general lack of normative data from the pediatric population against which to reference findings. To date, only a small number of studies have reported measures taken from uninjured cohorts. Despite the author groups concluding the need for additional research to develop a wider dataset of normative values, further efforts have been lacking.
The aim of this study therefore was to analyze upper cervical spine parameters in a pediatric cohort of patients without spinal column injury and thereby further add to our understanding of normative values.
Materials and Methods
Local ethical body approval was obtained for this study (HDEC: 20/STH/143). Due to the retrospective nature of this study, patient consent was not deemed necessary.
This study was performed at Waikato Hospital, New Zealand, a tertiary referral center for trauma for a population of nearly 1 million. The local radiology database was screened for both trauma CT and cervical spine CT performed on children aged ≤16 years from 2010 to 2019. All CT imaging was performed for major trauma assessment and obtained in line with Advanced Trauma Life Support principles. Dates were selected representing the availability of the digital imaging record. Images were excluded from analysis if there was osseous disease such as tumor, infection, or fracture, or if there was a diagnosis of spinal column injury either ligamentous or bony.
All CT images were accessed using Intellispace PACS Enterprise (Koninklijke Philips N.V.) and the linear measurement tool used for all measures. Age (months) and gender were recorded. Age was broken down into 2-year strata (8 subgroups) to allow further analysis and better determine any influence of age.
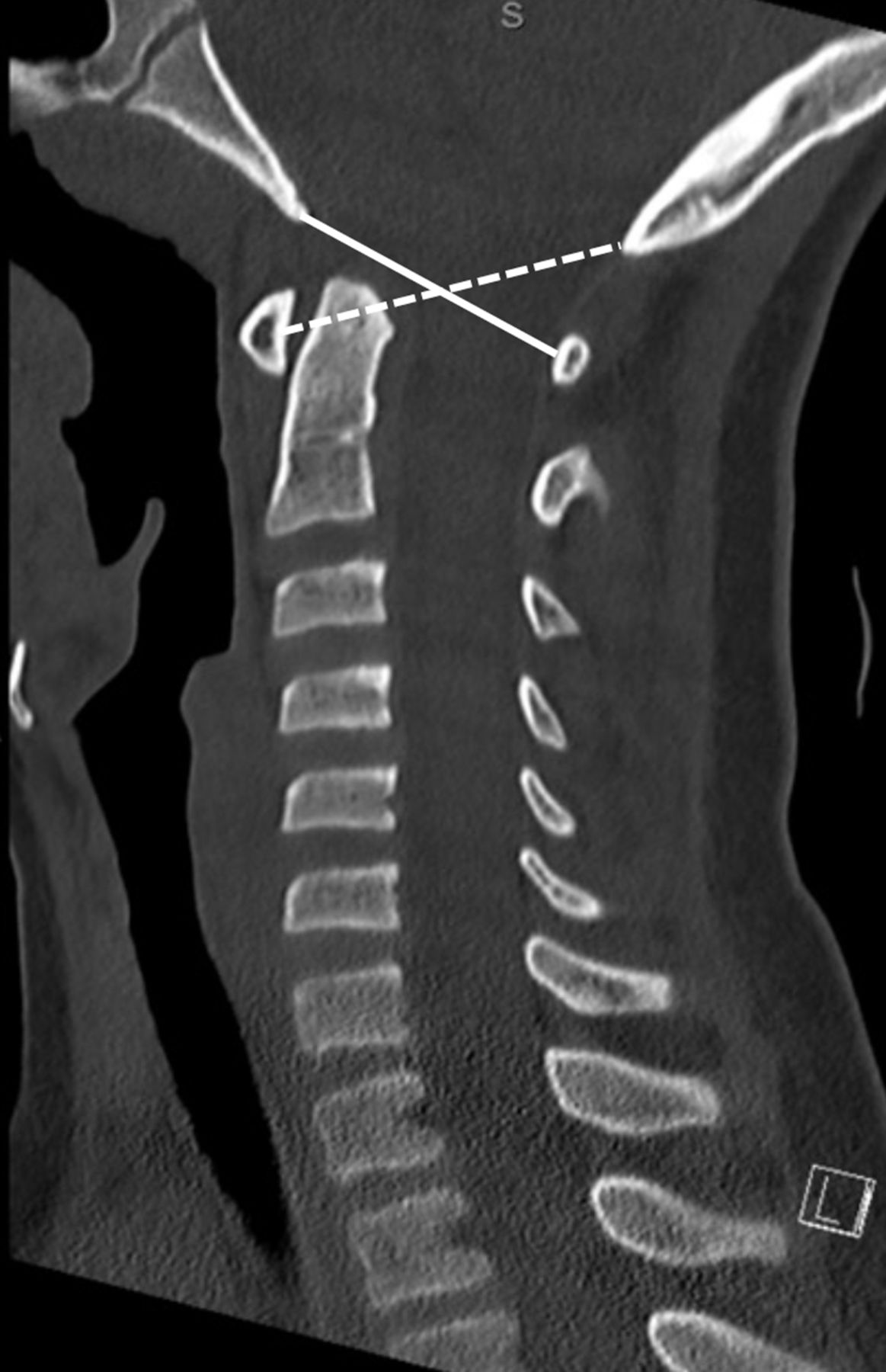
For each patient, selected measures that reflect potential ligamentous injury in the upper cervical spine were recorded. On the midsagittal image, the basion-dens interval (BDI), anterior atlanto-dens interval (ADI), posterior atlanto-dens interval (PADI), basion-to-C1 distance (B-C1), and opisthion-to-C1 distance (Op-C1) were measured (Figures 1 and 2). Measurement of the B-C1 and Op-C1 allowed calculation of the Powers ratio (B-C1/Op-C1).9

On the midsagittal image, the basion-dens interval (dashed line) is measured from the tip of the basion to the apex of the dens. The anterior atlanto-dens interval is measured between the posterior aspect of the anterior C1 arch and the anterior aspect of the odontoid process—the measurement is taken at the midpoint of C1. The posterior atlanto-dens interval is measured from the posterior aspect of the odontoid process to the anterior aspect of the posterior arch of C1.
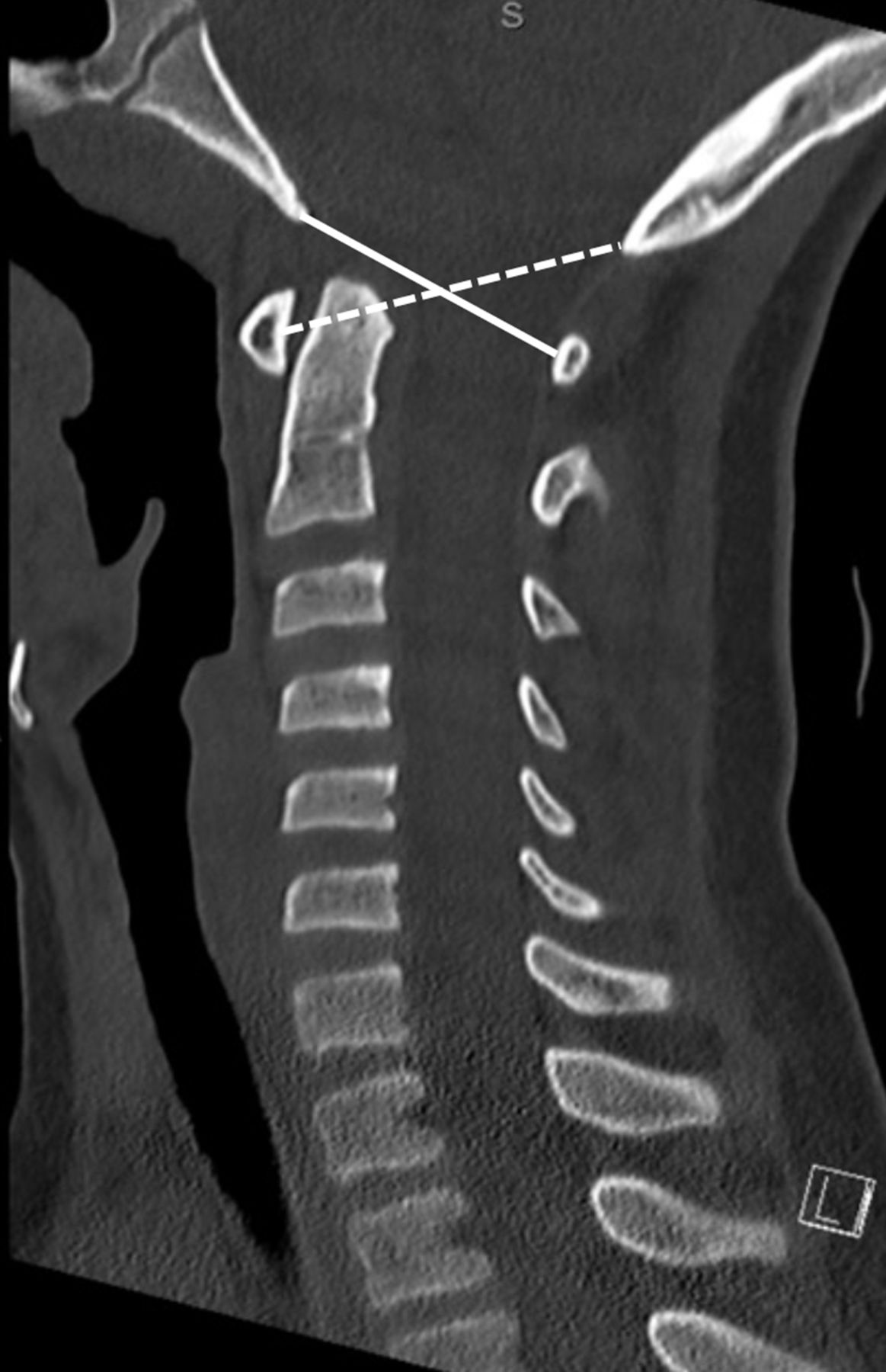
On the midsagittal image, the basion-C1 distance (B-C1) (solid line) is measured from the tip of the basion to the anterior aspect of the posterior arch of C1. The opisthion-C1 distance (Op-C1) (dashed line) is measured from the tip of the opisthion to the posterior aspect of the anterior arch of C1. The same C1 points were used for measuring the atlanto-dens interval and posterior atlanto-dens interval. To calculate the Powers ratio, B-C1 was divided by Op-C1 as well described.
The LMI and the condylar-C1 interval (CCI) were measured (Figure 3) on coronal images. The scout line function was used to determine the ideal coronal slice for each of CCI and LMI so as to allow measurement near the middle of the articulation on the corresponding image. For CCI, care was taken to avoid the sulcus visualized on the surface of the occipital condyle than can give an erroneously higher measurement. For LMI and CCI, measures were taken for each side.
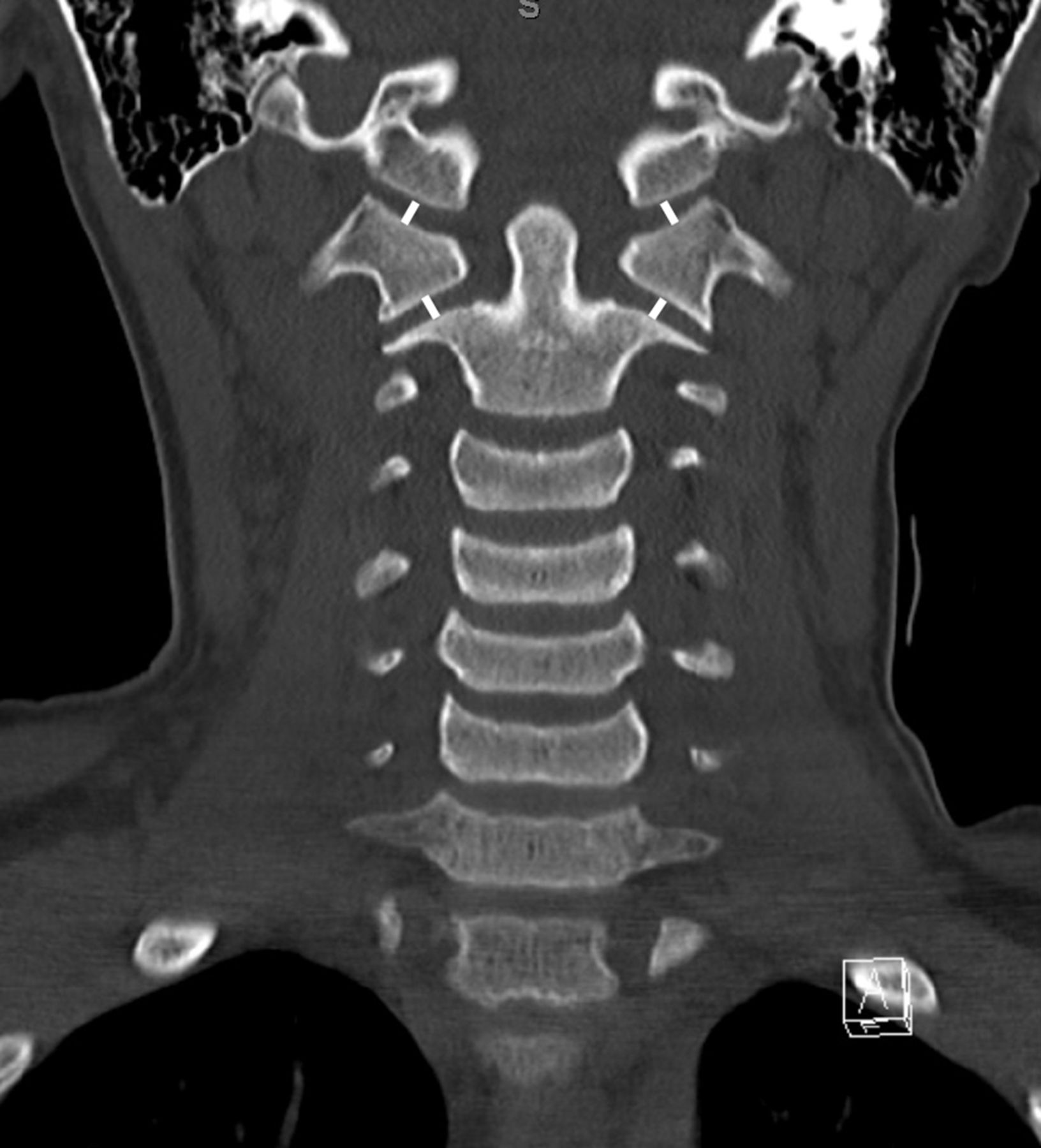
On the midcoronal image, the condylar-C1-interval is measured with a line in the middle of the joint drawn perpendicular to the joint surfaces; the lateral mass interval is drawn similarly with a line in the middle of the joint drawn perpendicular to the joint surfaces.
Inter- and intraobserver error has previously been reported to be moderate-high for all measurements. In this study, each measurement was recorded by a single fellowship-trained spine surgeon, and intraobserver error was calculated by repeating all measures on a subset of 10 patients at an interval of 8 weeks to allow sufficient washout. Cronbach’s α values for each of the measures were as follows: BDI 0.797; ADI 0.919; PADI 0.980; B-C1 0.941; Op-C1 0.973; CCI-r 0.922; CCI-l 0.875; LMI-r 0.881; and LMI-l 0.908.
Statistical Methods
All data were stored on Excel, and analysis was performed using ExcelSTAT. Mean, SD, and range are reported for all measurements. Shapiro-Wilk testing was used to determine the normal distribution of the data. Student t tests were used to compare values according to gender. R-values are reported from Pearson correlation analysis and one-way analysis of variance (ANOVA) used (Welch’s t test) to assess for differences in measurements between age cohorts. Linear regression analysis was used to assess the relationship between spinal measurements and age. A P value of <0.05 is statistically significant.
Results
One-hundred images were included in this study. There was a male predominance (62%). The mean age was 111.0 months (SD 51.0; range 11–196).
Mean values, SD, and range for each of the measurements from the cohort are shown in Table 1. Mean values, SD, and range for each of the measurements by gender are shown in Table 2.
Mean, SD, minimum, and maximum values for each of the variables collected.
Mean values by sex.
Pearson correlation analysis revealed a significant correlation between age and each of BDI
(−0.448; P < 0.0010), ADI (−0.201; P = 0.045), PADI (0.264; P = 0.008), B-C1 (0.547; P < 0.0001), Op-C1 (0.500; P < 0.0001), and both right and left CCI (−0.468; P < 0.0001 and −0.454; P < 0.0001). As the strength of association between each of B-C1 and Op-C1 and age was fairly similar, the resulting Powers ratio did not change with age. There was no significant correlation between age and LMI (−0.143; P = 0.16 and −0.081; P = 0.43).
Table 3 shows results, including ANOVA, of the study cohort considered in 2-year blocks. Mean and SDs are provided for the measurements in each cohort that can facilitate the calculation of desired confidence intervals. Significant differences between selected groups were evident for ADI, BDI, PADI, B-C1, Op-C1, Powers ratio, and CCI. BDI was significantly different between groups 3–4 and 7; ADI was different between groups 3–4 and 8; PADI was different between groups 3–8 and 1; Op-C1 different between groups 1 and 7–8; Powers ratio was different between group 1 and 3; CCI (both right and left) was different between groups 3 and 8; and LMI (left only) was different between group 1 and 4. Of all parameters, the Powers ratio remained the most consistent measure across the age groups (Figure 4).
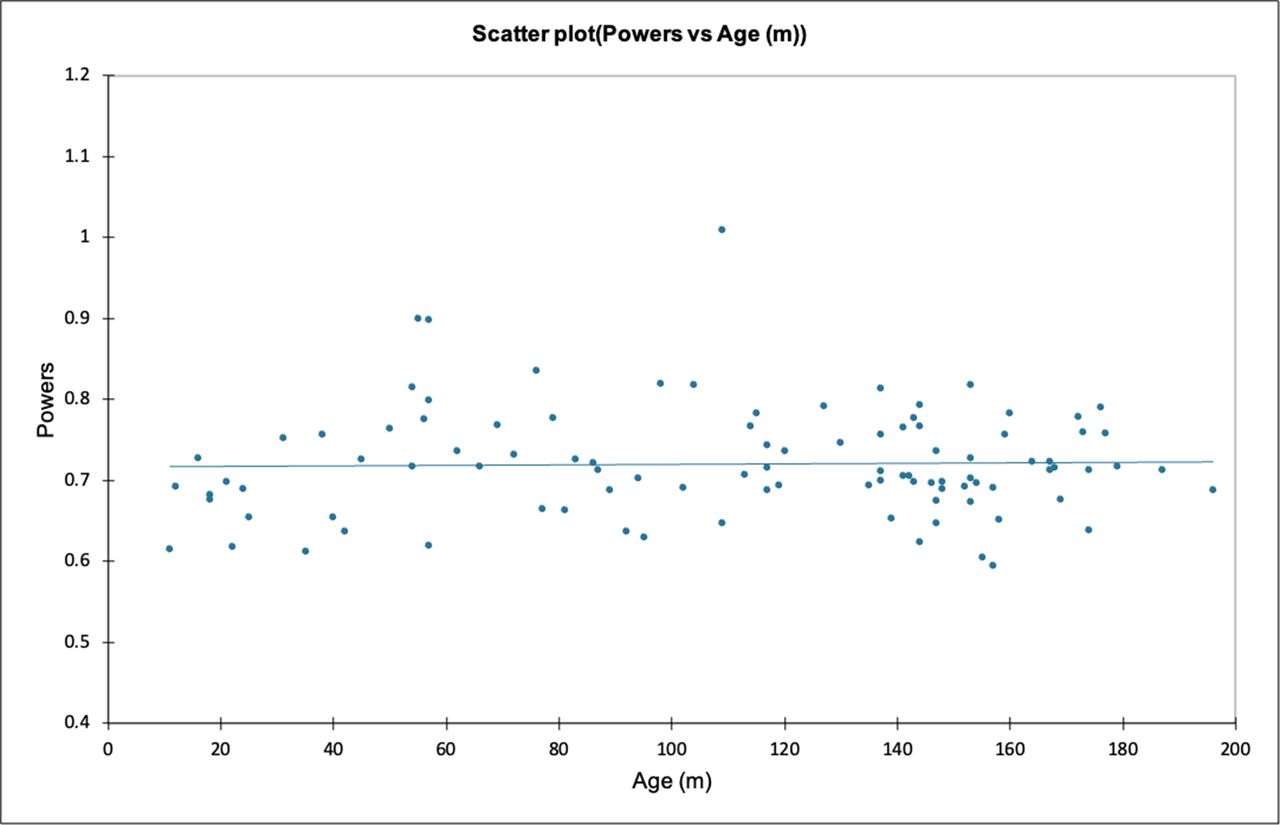
Scatter plot of the Powers ratio (y) plotted against age in months (x). Of all the measurements, the Powers ratio remained least variable across the age groups.
Results from 1-way analysis of variance (Welch’s test).
Linear regression analysis of each measurement against age (months) yielded the following equations:
Discussion
Injury patterns to the cervical spine within the pediatric population vary; in a cohort of 408 patients, Kokoska et al noted that younger children had higher injuries and were more likely to sustain dislocations, while older children had lower injuries and were more likely to sustain fracture.3 Similarly, Brown et al noted a higher rate of dislocation in the upper cervical spine in younger children than in older children, though they defined the upper cervical spine as C1-4 in their cohort of 103 patients.2 Finally, Platzer et al found that children aged 8 years or younger were significantly more likely to suffer an injury to the upper cervical spine than children aged over the age of 8 years.4 For clinicians, assessment and management of spinal injuries in the pediatric population can be challenging for multiple reasons, and a key component of assessment includes interpretation of advanced imaging.
This study adds further data to the literature on normative values for essential measurements when analyzing CT for a possible upper cervical spine injury in the pediatric population. A strength of this current study is the measurement of multiple parameters at once while previous authors have focused on one articulation or fewer parameters overall. The data are drawn from a population not previously studied, and mean values are provided for the different age cohorts stratified into 2-year blocks; confidence intervals can be determined from these values to provide upper limits of acceptability before mandating MRI or continued spinal precautions. Normative values from CT remain valuable in regions where MRI may still not be readily or widely available and also in the setting of assessing the obtunded or ventilated patient where obtaining MRI remains logistically difficult and early clearance of the cervical spine is desirable. This study provides increasing evidence that normative values vary with age throughout childhood and a “one size fits all” approach may not be appropriate.10 Understanding this potential for variation is essential when the measurements that may prompt additional investigation or influence treatment decision is crucial.
Condylar-C1 Interval
Normal values for the CCI have been reported by Pang et al previously in a cohort of 89 children.11 They utilized CT and measured the CCI on both the sagittal and coronal reconstructions. Measurements were taken at equidistant points along the joint on each side and the means obtained for sagittal, coronal, and combined measures. The mean value for the cohort was 1.28 ± 0.26 mm with no individual value exceeding 2.5 mm. Bertozzi et al have also reported on the CCI, measuring the atlantooccipital interval; in this instance, they measured the interval on sagittal images at 5 equidistant points along the joint yielding ranges of 0.4–3.1 and 0.5–3.3 mm on the left and right, respectively.12 These values are significantly different from those in the current study where the mean values for the right and left CCI were 2.0 and 2.0 mm, respectively, and the maximum values were 4.1 and 4.2 mm, respectively. Vachhrajani et al also found a higher mean value in their study.10 In 42 children aged from 1 to 214 months, the mean (SD) CCI was 2.38 (0.44) mm.
Whether this is related to the imaging acquisition or processing requires further exploration, and a major weakness of reports to date is the relatively small cohort sizes. It may also reflect the images chosen for measurement, the technique for measurement, and the use of a single measurement rather than selection of a number of equidistant points to generate a mean CCI.11,12 It is worth noting that the linear regression equation for CCI provided by Vachhrajani et al is very similar to that reproduced in this current study, and we noted a decrease in CCI with increasing age.10 This is in contrast to the findings of Pang et al who indicated that CCI and age did not correlate significantly.11
Powers Ratio
Powers et al reported on the eponymously termed ratio in 1979.9 This is easily determined by dividing the B-C1 distance by the Op-C1 distance; both these measurements correlated with age but similarly so, so the ratio itself is relatively constant throughout growth and in this study appeared the measurement with least variation across the age cohorts. Powers et al noted that a ratio of 1.0 occurs 2.6 SDs above the mean, so less than 1 % of the population should have a ratio greater than 1.0. In their study of normal CT images, Bertozzi et al similarly found a maximum ratio of 1.0.12 The findings from this current study are consistent with a maximum ratio of 1.0. Both the basion-C1 and opisthion-C1 distances are influenced by age to a similar degree, and thus the upper ratio that is acceptable should remain constant throughout childhood. A larger cohort would help estimate the proportion of the population that may have a ratio greater than 1.0, but over 40 years after its initial description, the Powers ratio remains of value. The reality is, however, that MRI is increasingly available, and any suspicion of a ligamentous injury will likely prompt additional investigation.
Basion-Dens Interval
Bertozzi et al studied 117 patients’ CT images and reported on the BDI finding mean values of 6.2 and 7.8 mm with ossification and without ossification of the os terminale, respectively.12 The maximum value recorded was 11.0 mm. In 97.5% of the cohort, the BDI was less than 10.5 mm—; this value is notably less than the values recorded on plain radiographs of 12 mm. Others have reported a mean value of 7.28 mm.10 The reported mean values are consistent in this current study although we note a slightly higher maximum value and we have not analyzed the influence of ossification of the os terminale. The timing of the appearance of the os terminale and its influence on the BDI require further clarification.
Anterior Atlanto-Dens Interval
The ADI was also studied by Bertozzi et al with a mean value of 1.4 mm reported and a range of 0.4–3.2 mm.12 Akturk and Gunes reported normative values from a cohort of 256 children.13 The mean ADI was reported to vary between 1.62 and 1.79 mm depending on the age group. Our study yielded a mean slightly higher than these reported values—again this is consistent with findings from Vachhrajani et al who also reported a mean (SD) ADI of 2.25 (0.24) mm.10 The mean age of this current cohort was older than that studied by Bertozzi et al (56 months) and Akturk and Gunes (92 months).12,13 Similar to CCI, therefore ADI changes with age and so larger cohorts are needed for refining normal values.
Posterior Atlanto-Dens Interval
The mean PADI reported by Vachrajani et al was 18.3 mm—very close to the 18.7 mm in this study.10 They noted again a correlation with age although not as strong as with other measures, and this is reflected in the findings from the ANOVA in this current study. The PADI is perhaps less utilized as the ADI is more commonly measured, and other measures taken in the sagittal plane provide the information that PADI does.
Lateral Mass Interval
The LMI has been reported previously by Rojas et al who measured the atlantoaxial joint space on coronal CT images.14 In their pediatric cohort of 112, they reported that more than 95% had an LMI of less than 3.9 mm on either side. A mean value for the entire pediatric cohort was not provided. In the current study, our results suggest that 95% would have a value less than 3.8 mm on either side. Vachhrajani et al reported a mean (SD) LMI of 2.91 (0.49) mm and an upper tolerance limit of 3.86. The maximum values for either left or right LMI in this current study are somewhat higher than the upper tolerance limit defined. As shown with linear regression, age may contribute to these differences with the mean age in this current study 11 months greater than that of Vachhrajani et al, while Rojas et al recruited children aged only up to the age of 10 years.10,14 Finally, Rojas et al used the mean value of the LMI taken at 3 points across the joint, while we have used only the center of the joint. When considering the morphology of the atlantoaxial articulation, the middle point of the 3 measurements as taken by Rojas et al would tend to be the largest, so this further explains the discrepancy.
Weaknesses in this study include a small cohort size but from a geographically separate and unique population compared to previous studies. A majority of images were obtained in children in the older age cohorts; images acquired in the very young, preambulatory phase comprise a very small portion, and so generating normative values for this particular cohort remains a challenge. In the absence of a multicenter study, generating a larger cohort may be challenging due to the relative rarity of advanced imaging being performed in this age demographic. As others have noted, it would be ideal to have a truly asymptomatic population to study, that is, imaging has been obtained without clinical need. This, however, raises a variety of ethical issues, none of which are easily overcome.
Although a relationship with age was shown, the correlation values were only moderate in strength at best, and so a larger cohort is needed to refine the linear regression equations provided. Other variables that could feasibly influence measurements (but were not considered) include body morphology and skeletal maturity. Data on height, weight, and body mass index were not readily available for this cohort; many patients underwent imaging but did not necessarily require inpatient hospitalization, so detailed observations were not filed. Skeletal maturity could be measured (a variety of ways) but would normally require a dedicated radiographic examination to accurately predict; this is an additional layer of complexity that could be considered in future prospective work but may not produce data that could be easily incorporated into clinical practice.
Future studies in this area need to use uniform techniques for measurement. Considering the CCI as an example, a variety of techniques have been used to measure this interval.10–12 While one technique may be more accurate than others to define anatomic limits, the ideal technique for measurement and clinical decision-making should also be easily used in day-to-day practice. To date, all studies have reported satisfactory reliability analyses.
Conclusion
In summary, this study adds further data to the literature regarding normative values for upper cervical spine measurements essential in assessing pediatric patients for possible ligamentous injury. It is clear that age influences the measurements, and so a standard upper limit cannot be applied to all patients skeletally immature without consideration for their age and skeletal maturity. Future efforts should draw on a larger population, across multiple centers, ensuring a wide age range to allow further definition of acceptable values to guide safe trauma assessment.
Footnotes
Funding The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The author reports no conflicts of interest in this work.
Ethics Approval Local ethical body approval was obtained for this study (HDEC: 20/STH/143).
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2022 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.