


Abstract
Background In an era of value-based medicine, patient-perceived benefit and satisfaction are of paramount importance. However, current metrics of success such as the minimal clinically important difference (MCID) do not always correlate with overall patient satisfaction. Therefore, the purpose of this study was to understand the relationships between self-reported pain, Oswestry Disability Index (ODI) scores, reaching the MCID, and overall patient satisfaction in patients undergoing elective lumbar fusions.
Methods A retrospective study including patients between the ages of 18 and 89 years old who underwent a 1- or 2-level elective lumbar fusion between June 2021 and June 2023. Patients were stratified using this overall level of satisfaction with their procedure. Differences in clinical metrics and patient-reported outcome scores among satisfaction levels were assessed, and predictive analytics were used to determine whether clinical metrics were associated with satisfaction.
Results A total of 343 patients were included in this study; 81% indicated they were satisfied with their overall outcomes. There were differences in both clinical metrics and patient-reported outcomes based on satisfaction level. Current pain and function were found to be independent predictors of satisfaction, while ODI scores and reaching MCID were not.
Clinical Relevance Relying on meeting statistically defined benchmarks of success, such as the MCID, may not provide an accurate depiction of procedural success or patient satisfaction, and additional clinically relevant benchmarks should also be assessed.
Conclusions Pain and current function were significantly associated with patient satisfaction; therefore, these metrics may play a larger role in patient satisfaction and perceived benefit than assessment through the ODI alone.
Level of Evidence 3.
Introduction
Health care spending and costs have risen substantially over the past few decades. Lumbar fusion procedures have increased by 63.3% from 2004 through 2015 within the United States, and during this period, the cost of a single-level lumbar fusion has risen 191%.1–3 Rising costs and increased utilization of health care services have prompted significant changes to move the United States Health Care System from a fee-for-service–based model to a value-based model.4–7 The central component in a value-based model is the idea of patient-perceived benefit. To measure perceived benefit, the Centers for Medicare and Medicaid Services, along with hospital accrediting bodies, now require the collection of patient-reported outcome (PRO) measures8,9 for at least 1 year postintervention to assess perceived benefit and value.7,10,11
Currently, perceived benefit is evaluated using a single statistically defined threshold value, the minimal clinically important difference (MCID). The MCID was initially proposed in 1989 as a means of normalizing a scoring system among various PRO measures to define the smallest change in score for which a patient would perceive some level of benefit.12 One of the most common disease-specific PRO measures to assess lower back pain and dysfunction is the Oswestry Disability Index (ODI).13–15 Initially developed in 1976, the ODI’s high degree of sensitivity and specificity has led to its widespread adoption. Despite the utility of PROs in both a clinical and research setting, these tools have a number of significant drawbacks. The necessary longitudinal data collection can be expensive and difficult; furthermore, missing data points and the potential for inadvertent selection bias can reduce the utility of PRO data in these settings. Recent studies have also suggested that the MCID can be significantly influenced by demographic and socioeconomic factors, as well as how the MCID threshold value is calculated.16–20 Given that the MCID is mostly devoid of clinical outcomes, it stands to reason that additional markers of success should also be investigated. Overall patient satisfaction has been suggested to be well correlated with the ODI scores of patients 3, 12, and 24 months after their surgical intervention.21 Therefore, this study seeks to better understand the relationships between clinical metrics (ie, postoperative pain reporting), patient-reported metrics for quality of life, ODI scores, reaching the MCID threshold for the ODI, and overall patient satisfaction in patients undergoing elective lumbar fusions.
Methods
This retrospective study was approved by the Institutional Review Board at our center. Patient records were included if the patients were aged between 18 and 89 years, underwent a 1- or 2-level elective lumbar fusion between June 2021 and June 2023, and completed the ODI within the 30 days preceding their indexed procedure, as well as completing both their 3-month postoperative ODI and overall procedural satisfaction. All PROs were collected using an online patient engagement platform (FORCE Therapeutics, New York, NY, USA). Patient records were excluded if the patients had undergone a fusion of 3 or more levels, a sacroiliac fusion, a spinal procedure without an associated fusion (eg, decompression or laminectomy), or a staged procedure or if they had a history of illicit drug use. Patient records were also excluded if their fusion was due to trauma or pathological condition (ie, cancer), if the patient was treated at an outpatient surgical center, if the patient had undergone another surgical procedure within 13 months of the index procedure, or if the patient’s insurance type was listed as worker’s compensation. Patients with worker’s compensation were excluded due to previous studies indicating significant differences in PRO scores based on insurance type,8 which is consistent with other published works.22
In addition to the ODI and satisfaction questions, patients at our institution were also asked to report their pain levels using a numeric pain scale at the time of hospital discharge as well as at 3 months postoperatively. A pain score of 0 indicated no pain, while a score of 10 indicated the worst pain possible. Patients were also asked to complete the patient-reported outcomes measurement information system global health 10 (PROMIS-10), a 10-question general health survey developed by the National Institute of Health to evaluate both physical and mental health, and compare the results to the United States population.23,24 For the purposes of this study, only the physical function subdomain T-score (PFT) of the PROMIS-10 was used in the analyses. The PROMIS-10 was chosen as a standard PRO at our institution both due to its relatively short construct as well as the subdomain measures and ease to compare to the United States population as a whole. The patient satisfaction question was in regard to the patient’s overall satisfaction with their surgical outcomes and was assessed using a 5-point Likert scale with 5 indicating extremely satisfied and 1 indicating extremely dissatisfied. For the purposes of this study, a score of 4 or 5 was considered satisfied, while a score of 3 or less was considered not satisfied.
Descriptive statistics were computed for all variables of interest. Continuous, normally distributed variables are presented as means and SD. Count-based data are presented as a percentage of the total study group. ODI scores, PROMIS-10 PFT, and pain scores were compared across the 5 levels of satisfaction using a single factor analysis of variance. Findings that were significantly different were further assessed using a Tukey post-hoc test to determine which groups were driving the statistically significant findings. Additionally, to determine the predictive nature of pain and PRO scores to patient satisfaction, nonparametric receiver operator curve (ROC) analysis was used, and an area under the curve value of 0.7 or greater was considered statistically significant. Statistically significant findings using the ROC analysis were followed up using a Youden J statistic to determine a cutoff threshold value. Finally, all factors identified as predictive of patient satisfaction using the ROC analyses were entered into a multivariate logistic regression model to determine which factors were independent factors associated with patient satisfaction. A P value of 0.05 or less was considered statistically significant. It is also important to note that, prior to the multivariate analysis, correlations were performed to ensure that none of the variables in the model were collinear.
Results
A total of 343 patient medical records were reviewed for the present study, and the majority of patients indicated that they were satisfied with their surgical outcomes, with 81.6% reporting that they were either extremely satisfied or satisfied with their outcomes. There were no significant differences in demographic or surgical variables among levels of satisfaction (Table 1).
Comparison of demographic and surgical data based on overall satisfaction levels.
There were no differences in preoperative PROs (neither the PROMIS-10 PFT nor the ODI), and there was no difference in pain levels at hospital discharge among satisfaction levels (Table 2). However, there were significant differences in both the 3-month postoperative values for each of the outcome variables as well as the change in scores between the pre- and postoperative time points among satisfaction levels (Table 2). There was also a significant difference in the number of patients reaching MCID based on overall satisfaction level (P = 0.008). A total of 57.6% of patients who reported being “extremely satisfied” met the published MCID threshold value for the ODI of 12.8,25,26 46.6% of patients reporting “satisfied” met MCID, and 30.6%, 25.0%, and 50.0% of patients reporting “neutral,” “dissatisfied,” and “extremely dissatisfied” met MCID, respectively.
Comparison of outcomes of interest by satisfaction level.
The results of the ROC analysis indicated that the variables of interest at 3 months after fusion as well as the change in pain levels were predictive of a patient indicating they were either satisfied or extremely satisfied (Table 3). The cutoff analysis indicated that patients with a PROMIS-10 PFT less than 38.4, a pain level greater than 5, and an ODI score greater than 23.8 at 3 months postoperative more likely indicated that they were unsatisfied with their outcomes. Additionally, patients reporting 1 point or less improvement in pain levels from their preoperative to postoperative state were more likely to be unsatisfied with their outcomes.
Results of the receiver operating characteristic analysis where the outcome was patient satisfaction.
The results of the multivariate logistic regression indicated that only the PROMIS-10 PFT at 3 months and change in pain level were independent predictors of patient satisfaction (Table 4). ODI scores, pain reporting at 3 months, and reaching MCID were not noted to be independent predictors of patient satisfaction. Results indicated that for every 1-point increase in patient-reported physical function, patients were 5% more likely to indicate that they were satisfied with their outcomes, and every 1-point reduction in pain level from hospital discharge to 3 months postfusion resulted in a 15% increased chance patients would indicate they were satisfied with their outcomes.
Results of multivariate logistic regression to determine independent predictors of patient satisfaction.
Discussion
In the era of value-based medicine, PROs have taken center stage as a means of determining procedural success and benefit to a patient. However, success following a surgical procedure can be nebulous in its definition, as success needs to be defined as a constellation of physical or functional outcomes, objectively measured clinical benchmarks, the results of PRO tools, and patient-perceived satisfaction. Currently, procedural success seems to be defined solely on patient attainment of the MCID—a statistically defined threshold value that can be limited in terms of clinical meaning. Recent studies have called into question the utility of the MCID given that its value can vary significantly based on demographic and socioeconomic variables, as well as how the MCID threshold value is calculated.16–20 Therefore, this study was designed to investigate how PROs scores, subjective reporting of pain, and attainment of the MCID impacted a patient’s overall satisfaction with the outcome of their 1- or 2-level elective lumbar fusion. The results of this study indicated that patient satisfaction was primarily influenced by 2 parameters: improvement in pain and the patient’s current level of physical function.
The results of the present study indicated that preoperative function as measured by the PROMIS-10 PFT and ODI were not associated with patient satisfaction. Additionally, it was noted that immediate postfusion pain was not associated with patient satisfaction. This constradicts somewhat with previous published literature that suggested that lower preoperative baseline scores were associated with greater postoperative improvement and thus increased patient satisfaction.27 Further contradicting previous studies was the fact that this study showed that patients in the “extremely satisfied” category started considerably better on the ODI than the “dissatisfied” group—and nearly the same as the “extremely dissatisfied” group—highlighting the variable nature of patient disease states.
The data in the present study suggested that ODI scores, on average, improved from the preoperative assessment to the 3-month postfusion assessment, with the greatest improvement in the “extremely satisfied” group and the least improvement in the “neutral group.” The ODI score change may not be directly correlated with patient satisfaction, which is consistent with previous studies that suggested self-reported physical function based on the ODI was not associated with patient satisfaction.28 However, PROMIS-10 PFT scores showed improvement in global function across all groups except those that were dissatisfied, which demonstrated almost no change to slightly worse function postoperatively; therefore, the PROMIS-10 PFT measure of overall function may be a better metric to assess improvements related to patient function and, consequently, satisfaction. Other studies have also suggested that the attainment of a patient’s preoperative goal has a significant influence on their satisfaction with surgical procedure.29,30 Although not measured in this study directly, patients starting out with worse function or greater levels of pain may have unrealistic goals associated with improvements in pain and function following surgery and thus lead to disappointment and lower levels of reported satisfaction. Therefore, preoperative discussions should involve setting proper patient expectations
The results of the ROC analyses demonstrated that when looking at the data dichotomously as either “satisfied” or “not satisfied” with surgical outcomes, all measures in this study at 3 months postfusion (ie, pain, ODI scores, and PROMIS-10 PFT) were predictors of patient satisfaction, while preoperative values were not. These findings make sense in the context that patient satisfaction takes into account current function and pain rather than past conditions prior to surgery. Additionally, the results of the logistic regression suggest that only changes in pain from pre- to postoperative assessments and overall physical function as assessed by the PROMIS-10 PFT were independent predictors of patient satisfaction. Pain levels themselves at 3 months postfusion, ODI scores, and attainment of the MCID for the ODI were not independent predictors. Therefore, the results suggest that current function and improvement in pain from their immediate postoperative state play a much more significant role in a patient’s satisfaction than reaching MCID or PRO-based metrics. These findings also point toward the need for additional metrics to be added to the current benchmarks of success to more accurately reflect the patient’s perceived benefit rather than using a single statistically derived metric as currently suggested.
Limitations
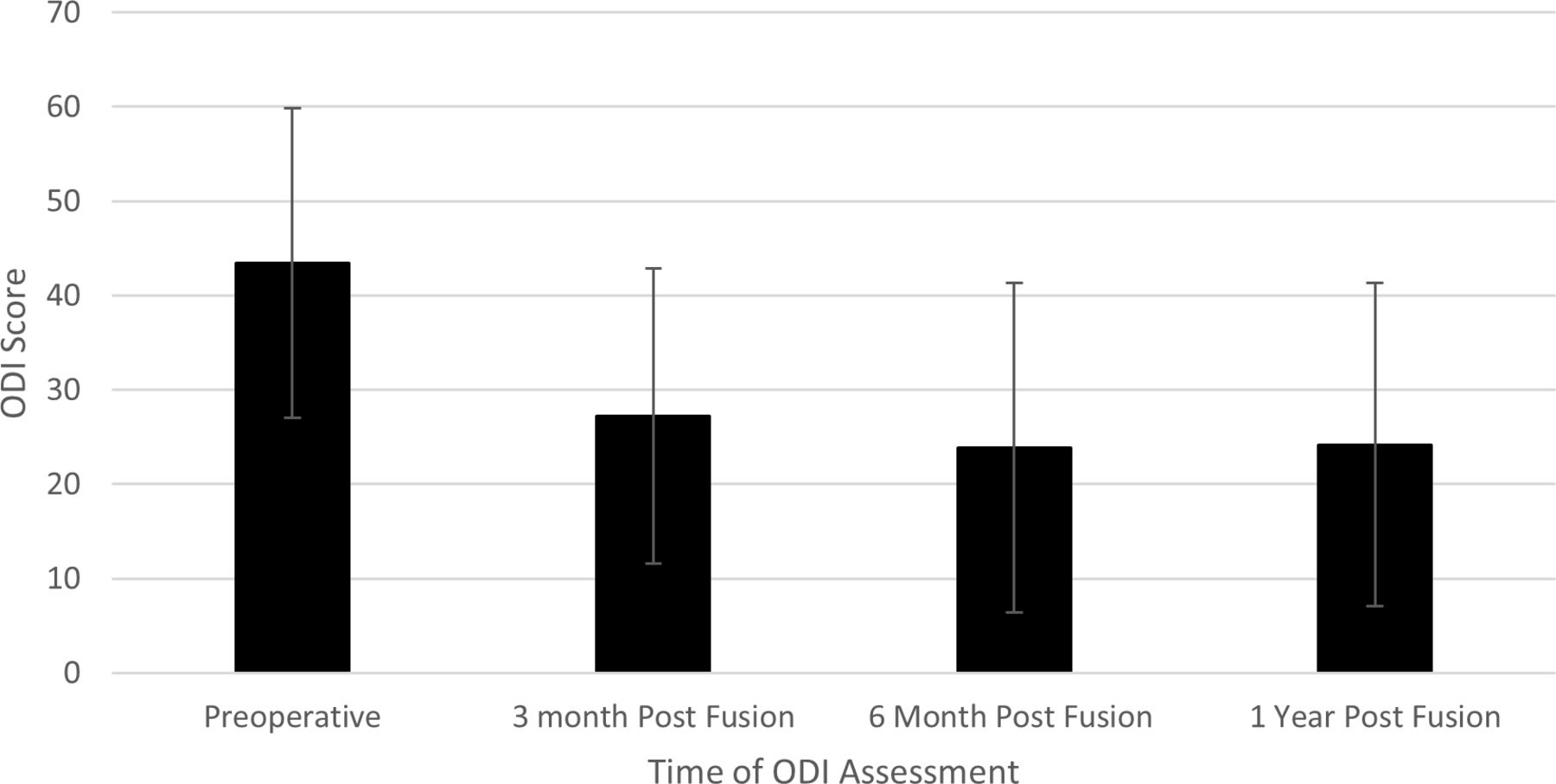
The present study was not without limitations. The study population was relatively homogeneous as indicated by the demographics and thus may not represent a generalizable sample. Additionally, the majority of patients in this study indicate that they were satisfied with their surgical outcomes, and a different population or studying a different procedure may yield alternative results. Further work should also look to see if the inclusion of Worker’s Compensation patients changes the results noted in this study. All data analyzed in this study were based on 3-month post-fusion data, given that our institutional standard of care is to collect overall satisfaction only at a single time point—12 weeks following their index procedure—and thus, results may change further out from surgery. Furthermore, the patient sample used in this study completed all PROs at both their preoperative and 3-month postoperative assessments, and therefore, this inclusion criteria may have led to unintended selection bias. Additionally, this study used 3-month data only, as data indicated limited to no change in ODI and PROMIS-10 scores following the 3-month assessment in this patient cohort (Figure); however, the data presented in this work represent only outcomes at 3 months and should not be extrapolated to later time points. It is also important to note that clinical metrics were not included as outcomes (ie, fusion rates or complication rates). This was an intentional decision, given that complications are quite rare and, furthermore, patient satisfaction may be a better hallmark of success than a radiographic finding or the absence of complications.

Oswestry Disability Index (ODI) score trends from the preoperative to 1-year postoperative assessment. Black bars represent the mean, while the error bars are ±1 SD.
Conclusion
In the present study, improvement in pain and current function was significantly associated with patient satisfaction. In the era of value-based medicine, which emphasizes disease-specific PRO scores and attaining statistically defined benchmarks of success such as the MCID, this study suggests that success for patients who underwent 1- or 2-level lumbar fusion cannot solely be judged by current metrics alone. The benefit to the patient may also need to include evaluations of both improvement in pain and current functional status beyond what is currently evaluated using legacy PROs such as the ODI.
Footnotes
Funding The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests The authors report no conflicts of interest in this work.
IRB Statement This study was approved by the Hartford Hospital Institutional Review Board.
- This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2025 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.